MACRA Glossary
To understand MACRA basics and nail down the details required to navigate the Quality Payment Program (QPP), we’ve compiled this comprehensive MACRA glossary of essential terminology that pertains to federal health reporting programs. The terms below are grouped by related topics, or areas of the QPP, for better comprehension of the subject matter.
Recently updated for 2020, this resource will continue to evolve to keep pace with evolving MACRA regulations and requirements.
What Is MACRA?
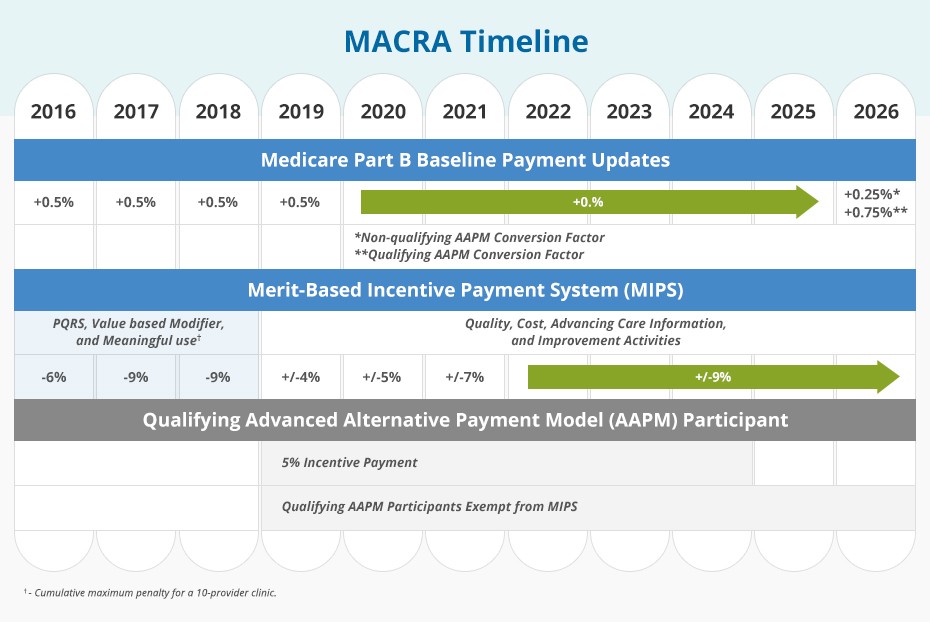
MACRA is an acronym for the Medicare Access and CHIP Reauthorization Act of 2015, a law that reformed the Medicare Part B payment system by repealing the Sustainable Growth Rate (SGR) formula used to update the Medicare Physician Fee Schedule (MPFS).
MACRA replaced the SGR with a “value-based” payment system with the goal of improving the quality of healthcare and patient outcomes and rewarding providers who achieve these ends while maintaining or lowering costs. MACRA also reauthorized the Children’s Health Insurance Program (CHIP).
What Is the Quality Payment Program (QPP)?
The Quality Payment Program (QPP) is a Centers for Medicare & Medicaid Services program developed to comply with MACRA. Consolidating and building upon multiple quality measurement and reimbursement legacy programs, the QPP is designed to move healthcare providers from a fee-for-service reimbursement paradigm to a value-based payment system.
The objective of the QPP is to implement a patient-centered healthcare system that achieves improved care, strategic spending, and better patient outcomes. Eligible clinicians can choose how to participate—based on practice size, specialty, location, or patient population—and will be rewarded for providing higher-value care.
Who Is a MIPS Eligible Clinician?
A MIPS eligible clinician is a healthcare provider who meets Quality Payment Program (QPP) participation criteria and is therefore eligible to participate (or subject to mandatory participation) in the Merit-Based Incentive Payment System (MIPS)—one of Medicare’s QPP tracks.
MIPS eligible clinicians include physicians, physician assistants, nurse practitioners, clinical nurse specialists, certified registered nurse anesthetists, chiropractors, dentists, podiatrists, optometrists, osteopathists, physical therapists, occupational therapists, qualified speech-language pathologists, qualified audiologists, clinical psychologists, and registered dieticians or nutrition specialists—provided they meet or exceed the low-volume threshold.
What Is the Low-Volume Threshold for MIPS Participation?
The low-volume threshold is the criteria eligible clinicians must meet to participate in the Merit-Based Incentive Payment System (MIPS) and qualify for MIPS payment adjustments.
As defined by the Centers for Medicare & Medicaid Services, for the 2020 performance year, clinicians, groups, and MIPS APM entities are excluded from MIPS if, during either segment of the MIPS determination period, they bill Medicare for less than or equal to $90,000 in Medicare Part B allowed charges, or provide care for200 or fewer Medicare Part B beneficiaries, or provide 200 or fewer Medicare Part B covered professional services under the MPFS.
Clinicians who meet or exceed one or two of the low-volume threshold criteria, however, can opt in to participate in MIPS. Additionally, a clinician excluded as an individual due to the low-volume threshold may be eligible to participate if the clinician’s practice reports as a group or virtual group.
What Is the MIPS Determination Period?
As of Year 3 (2019), MIPS eligibility is determined based on two consecutive 12-month look-back periods that align with the fiscal year (although eligibility is based only on the first 12-month period). For 2020, the two determination periods are Oct. 1, 2018, to Sept. 30, 2019, and Oct. 1, 2019, to Sept. 30, 2020.
Who Are Non-Patient Facing MIPS Eligible Clinicians?
A non-patient facing MIPS eligible clinician is a clinician who meets or exceeds the low-volume threshold but only bills Medicare for 100 or fewer patient-facing services (including telehealth services) under Medicare Part B during one or both of the 12-month segments of the MIPS determination period. Groups and virtual groups also qualify for this special status when more than 75% of the clinicians in the group or virtual group are non-patient facing eligible clinicians. Non-patient facing eligible clinicians are afforded more flexible reporting options under MIPS.
What Is a New Medicare-Enrolled MIPS Eligible Clinician?
A new Medicare-enrolled MIPS eligible clinician is a professional who enrolls in Medicare through the Provider Enrollment, Chain, and Ownership System (PECOS) for the first time during the performance period.
The new Medicare-enrolled MIPS eligible clinician has not, under any billing number or tax identifier, previously submitted a claim as a Medicare-enrolled EC, either as an individual or as part of a group.
What Is a Small Practice in Terms of QPP Participation?
A small practice is defined by the Centers for Medicare & Medicaid Services as a practice with 15 or fewer clinicians with national provider identifiers (NPIs) billing under the same Taxpayer Identification Number (TIN).
What Is a MIPS Virtual Group?
A MIPS virtual group is a combination of two or more Taxpayer Identification Numbers (TINs) assigned to one or more solo practitioners or groups, each consisting of 10 or fewer eligible clinicians (with at least one being a MIPS eligible clinician), that choose to form a virtual group for a performance year for the purposes of participating in the Merit-Based Incentive Payment System (MIPS) under a single TIN.
What Is MIPS?
The Merit-based Incentive Payment System (MIPS) is one of two payment tracks of the Quality Payment Program (QPP). Under MACRA, MIPS consolidates the Physician Quality Reporting System, Value-Based Payment Modifier Program, and Medicare Electronic Health Records Incentive Program into a single program.
Eligible clinicians participating in MIPS are scored and rewarded in accordance with requirements outlined for Quality, Cost, Improvement Activities, and Promoting Interoperability performance categories.
What Is a MIPS Performance Category?
A MIPS performance category is one of four categories—Quality, Cost, Improvement Activities, and Promoting Interoperability—that form the basis of the Merit-Based Incentive Payment System (MIPS) tract of the Quality Payment Program. Each category is weighted and contributes to a MIPS eligible clinician’s or group’s final score. Performance category weights can vary by year as the program evolves.
What Is the MIPS Quality Performance Category?
The MIPS Quality performance category requires eligible clinicians to collect and report quality measure data. The quality component of MIPS is the highest weighted performance category, worth 40% of a MIPS final score in the 2020 performance year. For performance year 2020, MIPS participants must choose six quality measures (from over 206 quality measures) on which to report.
How Do You Calculate the MIPS Quality Performance Category Score?
Six quality measures are required for full compliance in the Quality performance category. Each measure is worth up to 10 points. The maximum quality score, therefore, is 60 points. Measures are scored in decimals based on data completeness compared to national benchmarks.
To calculate the MIPS quality score for individual reporters, or when the All-Cause Hospital Readmission measure does not apply, add of the total points earned for each measure reported, divide that number by the total possible points (60). Multiply the resulting percent by weight of category (40%) and then by total possible score (100). The result is your score in the Quality performance category.
Total Points Earned / 60 = Percent of Quality Earned
Percent of Quality Earned x 40% x 100 = MIPS POINTS
What Are Clinical Quality Measures?
Clinical quality measures (CQMs) are tools for assessing and tracking observations, treatment, processes, experience, and outcomes of patient care. CQMs also offer one option for individual MIPS data submission.
What Is a High-Priority Measure?
A high-priority measure is a MIPS quality measure within one of the following categories: outcome, appropriate use, patient safety, efficiency, patient experience, care coordination, or opioid-related measures.
MIPS eligible clinicians are required to report at least one outcome measure or high-priority measure to achieve the highest score in the Quality performance category (60 points). Although a final MIPS score cannot exceed 100%, MIPS eligible clinicians can earn extra credit, adding 1 bonus point to a final MIPS score for every additional high-priority measure reported. (As of 2019, MACRA Year 3, CMS Web Interface reporters no longer earn high priority measure bonus points.)
What Is the All-Cause Hospital Readmission Measure?
The All-Cause Hospital Readmission is the measure of readmission rate of patients age 65 or older who experience an unplanned hospital readmission within 30 days of discharge following a short-stay acute care hospitalization.
This measure is calculated by CMS using administrative claims and is included in the MIPS quality performance category. The All-Cause Hospital Readmission measure only applies to groups of 16 or more eligible clinicians with at least 200 cases. No data submission from clinicians is required.
What Is the MIPS Cost Performance Category?
The MIPS Cost performance category measures eligible clinicians and groups on the resources used to treat attributed Medicare beneficiaries. Cost performance is based on Medicare Part B claims data and measures, and accounts for 20% of a MIPS final score in the 2020 performance year.
To calculate the Cost performance category percent score, divide the number of points assigned to the measure (based on performance, compared to the national benchmark) by the number of total possible cost achievement points available, and then multiple by 100.
Unlike the other performance categories in the Merit-Based Incentive Payment System (MIPS), the Cost performance category requires no reporting by MIPS eligible clinicians and groups. MIPS eligible clinicians will be awarded points based on their cost performance against measure benchmarks. In MACRA Year 4 (2020), Cost performance category measures include:
Total per Capita Cost measure
Medicare Spending per Beneficiary measure
Episode-based measures
What Is Attribution or Attributed Beneficiaries?
Attribution is the process used by Medicare (and commercial payers) to assign patients to the physicians who are held accountable for their care. MACRA dictates specific attribution methods for the two participation tracks of the Quality Payment Program (QPP).
Attribution within the Merit-Based Incentive Payment System (MIPS) (track 1) uses Taxpayer Identification Numbers (TINs), not National Provider Identifiers (NPIs). Eligible clinicians are incentivized to see patients more frequently who are attributed to them. Advanced APMs (track 2 of the QPP) have different rules on what constitutes a patient as “attributed” to a provider.
What Is Total Per Capita Cost (TPCC)?
Total per Capita Cost (TPCC) is a claims-based measure of overall efficiency of care provided to attributed patients used in the Cost performance category of MIPS. The formula looks at the overall cost of a patient’s care for both Medicare Parts A and B.
TPCC measures the total yearly costs for all patients assigned to a provider, divided by the total number of patients assigned to that provider. Beginning in 2020, TPCC attribution will require evaluation and management (E/M) services to have an associated primary care service or a follow-up E/M service from the same clinician group. Eligible clinicians will be scored on TPCC if they meet the case minimum, which is set at 20. Certain clinicians who deliver mostly non-primary care services might also be excluded from TPCC.
What Is the Medicare Spending Per Beneficiary?
The Medicare Spending per Beneficiary (MSPB) is a claims-based measure in the Cost performance category of the Merit-Based Incentive Payment System (MIPS). This resource-use measure is triggered by acute care episodes related to hospitalizations and includes all Parts A and B payments beginning two days prior to hospitalization and lasting for 30 days following hospitalization. The MSPB measure applies to clinicians with a minimum of 35 cases.
What Is an Episode-Based Measure?
An episode-based measure is based on services provided to a patient during an episode of care covered under Medicare Parts A and B that are related to a triggering condition or procedure. Clinical and treatment episode-based measures evaluate resource utilization of certain costly and prevalent procedures and conditions.
Episode-based measures require a case minimum of 10 for procedural episodes and a case minimum of 20 for acute inpatient medical condition episodes. For procedural episodes, the Centers for Medicare & Medicaid Services (CMS) will attribute episodes to each MIPS eligible clinician who renders a trigger service (identified by procedure codes). For acute inpatient medical condition episodes, CMS will attribute episodes to each MIPS eligible clinician who bills inpatient evaluation and management (E/M) services claim lines during a trigger inpatient hospitalization under a TIN that renders at least 30% of the inpatient E/M claim lines in that hospitalization.
What Are Quality and Resource Use Reports (QRURs)?
Quality and Resource Use Reports (QRURs) are provided to every group practice and solo practitioner based on their Taxpayer Identification Number (TIN). Reviewing this report, which shows how clinicians and groups performed on quality and cost measures, is a valuable way to understand cost and quality performance in preparation for the Quality Payment Program (QPP).
What Are Supplemental Quality and Resource Use Reports?
Supplemental Quality and Resource Use Reports (sQRURs) are informational only and provide payment-standardized, risk-adjusted cost information on episodes of care provided to Medicare patients. Reviewing this report is key to becoming familiar with the episode-based resource use measurement that impacts eligible clinicians’ scores in the Merit-Based Incentive Payment System (MIPS).
What Are Improvement Activities?
Improvement activities is a performance category under the Merit-Based Incentive Payment System (MIPS) and are identified as improving clinical practice or care delivery that likely results in improved patient outcomes. Improvement activities focus on care coordination, beneficiary engagement, and patient safety.
For Year 4 (2020) of MIPS, there are two new activities, modifications to seven existing activities, and 15 activities are removed. This category is worth 15% of the MIPS final score. To get full credit, a clinician or group must complete activities equal to a maximum 50 points or participate in a Patient-Centered Medical Home, Medical Home Model, or similar specialty practice and a MIPS APM.
What Is a Patient-Centered Medical Home?
A Patient-Centered Medical Home (PCMH) is a model of the organization of primary care that delivers the essential functions of primary healthcare defined as patient centered, comprehensive, team-based, coordinated, accessible, and focused on quality and safety.
The goal of PCMH is to provide patients with necessary and appropriate care when and where they need it, in a manner they can understand. Ideally, care is coordinated by registries, information technology, and health information exchange. Eligible clinicians under a Taxpayer Identification Number (TIN) where at least 50% of the practice sites are certified PCMHs will receive full credit in the Improvement Activities performance category.
What Is Promoting Interoperability?
Promoting Interoperability is a MIPS performance category (formerly called Advancing Care Information) that requires the meaningful use of certified electronic health record technology (CEHRT). The intention driving this MIPS performance category is to create a patient-driven healthcare system where patients have the information needed to become active healthcare consumers.
As with Meaningful Use the Promoting Interoperability performance category continues the effort for the secure exchange of protected health information. For most providers, this category is worth 25% of their MIPS final score. In some cases, a provider may qualify for an exception from this category. In these circumstances, the Promoting Interoperability performance category will be reassigned a weight of 0%, and the weight of the Quality performance category will be increased—from 40% to 65% (in performance year 2020).
What Is CEHRT?
CEHRT is an acronym for certified electronic health record technology. The Centers for Medicare & Medicaid Services (CMS) and the Office of the National Coordinator for Health Information Technology (ONC) have established standards and other criteria that define the technological capability, functionality, and security required for electronic health record (EHRs) technology.
CEHRT gives assurance to clinicians and patients that the electronic health IT products and systems they use are secure, can maintain data confidentially, and can work with other systems to share information. Certification of EHR products is done by ONC. As of Year 3 (2019) of the Quality Payment Program (QPP), providers must use 2015 CEHRT to participate in the QPP. Unlike previous years, in 2019 and beyond, eligible clinicians do not earn bonus points in the Merit-Based Incentive Payment System for 2015 CEHRT use.
What Is a Qualified Clinical Data Registry (QCDR)?
Qualified Clinical Data Registry (QCDR) is an entity approved by CMS that collects medical and clinical data for patient and disease tracking to promote better quality of care and ongoing improvement to medical treatments and services provided to patients. Among various methods for reporting MIPS quality performance data, MIPS eligible clinicians, groups, and virtual groups may submit data using a QCDR. The QCDR will complete the collection and submission of quality measures data on behalf of the MIPS eligible clinician or group.
What Is a MIPS Score?
A MIPS score, or MIPS performance score, is one of four scores you will receive for your performance in each MIPS category. Your scores will be based on how well you conduct activities specified within each MIPS performance category. The individual MIPS performance category scores are then aggregated to produce a MIPS final score.
What Is a MIPS Final Score?
A MIPS final score is a composite performance score of a provider’s cumulative scores in the Merit-Based Incentive Payment System (MIPS), achieved in the four performance categories—Quality, Cost, Improvement Activities, and Promoting Interoperability. The MIPS final score is then compared to the CMS performance threshold score for a given year to benchmark performance relative to all MIPS physicians.
Individual performance scores are weighted differently in the calculation of a MIPS final score. In 2020, the weights are 20% for cost, 40% for quality, 15% for improvement activities, and 25% for promoting interoperability.
An eligible clinician’s or group’s MIPS final score determines the percentage adjustment applied to their Medicare Part B claims during the payment year. Incentive adjustments to payments resulting from the individual’s or group’s MIPS final score are received in the second calendar year following the performance year.
What Is a Measure Benchmark?
A measure benchmark is an empirical level of performance (the mean performance of total participants) on which a MIPS eligible clinician will be assessed. Quality benchmarks have a two-year look back period, while cost benchmarks are determined during the performance period.
What Is a Topped-Out Measure?
A topped-out measure is a measure where the overall performance is so high or unvarying that meaningful distinctions and improvements cannot be made by most MIPS eligible clinicians. Each annual Medicare Physician Fee Schedule final rule identifies these measures. When a measure is identified as topped out for three consecutive years, it is eliminated in the fourth year.
What Is the MIPS Performance Threshold?
The MIPS performance threshold is the minimum points eligible clinicians need to earn to avoid receiving a negative payment adjustment. In performance year 2020, MIPS eligible clinicians will need to earn a final score of at least 45 points to avoid a payment reduction of up to negative 9% in payment year 2022. This increase reflects a steady rise from the 2018 15-point threshold and the 2019 30-point threshold.
What Is the Payment Adjustment Factor?
A payment adjustment factor, also known as the MIPS adjustment factor, is the percentage adjustment applied to a MIPS eligible clinician’s Medicare Part B payments. The adjustment factor is based on a linear sliding scale and results in differential payments.
As required by law, the payment adjustment for the 2022 payment year ranges from minus 9% to plus 9% x scaling factor. The scaling factor is determined to achieve budget neutrality.
Payment adjustments are applied two calendar years after the performance year, so a MIPS eligible clinician will receive a payment adjustment in 2022 based on their 2020 performance.
Qualifying Alternative Payment Model Participants (QPs) receive a lump sum incentive payment equal to 5% and are not subjected to the MIPS adjustment factor.
What Is Budget Neutrality?
Budget neutrality is a MACRA requirement that ensures the financial sum of positive payment adjustments made through the Quality Payment Program (QPP) does not surpass the financial sum of negative payment adjustments. The QPP accomplishes this by funding positive payment updates from the cache of negative payment updates.
What Is a Payment Year for MACRA QPP Participation?
A payment year in MACRA’s Quality Payment Program (QPP) is the calendar year when payment adjustments are made to a QPP participant’s Medicare Part B payments. The payment year occurs two years after the performance year on which the payment adjustments are based. For QPP participants that began participation in 2017, their first QPP payment adjustment occurred in 2019.
What Is Exceptional Performance?
Exceptional performance is a Merit-Based Incentive Payment System (MIPS) incentive that rewards MIPS eligible clinicians who meet or exceed the exceptional performance threshold. MIPS eligible clinicians who are exceptional performers will receive an additional positive payment adjustment to their Medicare Part B claims payment, which is capped at 10% and made on a sliding scale based on performance.
To receive an exceptional performance bonus for 2020 (payment year 2022), will require a MIPS eligible clinician to earn a minimum of 80 points in their MIPS final score, up from 75 points in 2019. The exceptional performance threshold in 2021 will be 85 points.
With an additional $500 million allocated for exceptional performance payments, this bonus incentive falls outside budget neutrality requirements of MIPS. The adjustment for exceptional performance, however, is only available from 2019 to 2024.
What Is an Alternative Payment Model (APM)?
An Alternative Payment Model (APM) is an approach to paying for healthcare through Medicare that incentivizes quality and value. APMs represent one of two payment tracks under MACRA’s Quality Payment Program. Examples of APMs include Medicare Shared Savings Program (MSSP), accountable care organizations (ACOs), patient-centered medical homes, bundled payment models, and other initiatives.
What Is a Qualifying APM Participant (QP)?
A Qualifying Alternative Payment Model Participant (QP) is an eligible clinician who receives a percentage threshold of patients or payments through an APM during the performance period. QPs are eligible to receive a lump sum incentive payment equal to 5% through 2024 and are exempt from MIPS.
The Centers for Medicare & Medicaid Services (CMS) will recognize clinicians as QPs if they appear on and Advanced APM’s Participation List during a “snapshot” period (March 31, June 30, and August 31, as well as December 31 for Medicare Shared Savings Program participants). Clinicians not participating in an Advanced APM during at least one of these “snapshots” will need to submit data to MIPS using the MIPS individual or group options to avoid a negative payment adjustment. MIPS APM special scoring may apply.
Beginning in 2019, CMS allows for QP determinations under the All-Payer Option to be requested at the TIN level, in addition to the APM entity and individual eligible clinician levels, when all eligible clinicians who have reassigned their billing rights to the TIN are included in a single APM entity.
Payment Year | 2021 | 2022 | 2023 and Later |
|---|---|---|---|
QP Payment Amount Threshold | |||
Medicare Minimum | 25% | 25% | 25% |
Total | 50% | 50% | 75% |
QP Patient Count Threshold | |||
Medicare Minimum | 20% | 20% | 20% |
Total | 35% | 35% | 50% |
What Is a Partial QP?
A Partial QP is an eligible clinician who participates in an Advanced Alternative Payment Model (APM) but hasn’t met the payment or patient threshold to be considered a Qualifying APM Participant (QP). A Partial QP is ineligible to receive the 5% lump sum bonus. If the Advanced APM is a MIPS APM, and the Partial QP opts to participate in MIPS, the Partial QP will be scored under the APM Scoring Standard.
MIPS eligible clinicians can check their QP status using the QPP Participation Status Tool.
Payment Year | 2021 | 2022 | 2023 and later |
|---|---|---|---|
Partial QP Payment Amount Threshold | |||
Medicare Minimum | 20% | 20% | 20% |
Total | 40% | 40% | 50% |
Partial QP Patient Count Threshold | |||
Medicare Minimum | 10% | 10% | 10% |
Total | 25% | 25% | 35% |
What Is the APM Scoring Standard?
The APM Scoring Standard is used for MIPS eligible clinicians who are Partial Qualifying APM Participants (Partial QPs) in a MIPS APM and who have elected to participate in MIPS. Under the APM Scoring Standard, the categories and weights of the performance categories differ from the categories and weights for MIPS eligible clinicians.
A MIPS final score will be aggregated at the APM entity level based on scores of MIPS eligible clinicians in the APM entity.
What Is a MIPS APM?
MIPS APMs are Alternative Payment Models (APMs) that meet three criteria:
APM entities must participate in the APM under an agreement with CMS.
APM entities must include at least one MIPS eligible clinician on a Participation List.
APM entities must base payment incentives on performance, quality measures, and cost/utilization.
MIPS eligible clinicians participating in a MIPS APM and MIPS receive special scoring considerations under the APM Scoring Standard.
It is possible for an APM to have tracks that are MIPS APMs and tracks that are not MIPS APMs. All Advanced APMs are also MIPS APMs. CMS expects the following 10 APMs to meet MIPS APM requirements for the 2020 performance period:
Comprehensive ESRD Care Model (all tracks)
Comprehensive Primary Care Plus (CPC+) Model (all tracks)
Next Generation ACO Model
Oncology Care Model (all tracks)
Medicare Shared Savings Program (all tracks)
Medicare ACO Track 1+ Model
Bundled Payments for Care Improvement Advanced
Maryland Total Cost of Care Model
Vermont All-Payer ACO Model
Primary Care First (all tracks)
Independence at Home Demonstration
What Is a Physician-Focused Payment Model?
Physician-focused payment models (PFPMs) are Alternative Payment Models established by physicians under the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA). The Physician-Focused Payment Model Technical Advisory Committee (PTAC) makes recommendations on PFPMs to the Secretary of the Department of Health and Human Services.
What Is Physician-Focused Payment Model Technical Advisory Committee (PTAC)?
Physician-focused Payment Model Technical Advisory Committee (PTAC) is the body that reviews recommendations on PFPMs submitted by stakeholders. The secretary of the Department of Health and Human Services (HHS) must establish, through notice and comment rulemaking, criteria for PFPMs, which include models for specialist physicians that could be used by the PTAC for making its comments and recommendations.
What Is a Bundled Payment Model?
A bundled payments model is one type of alternative payment model (APM) where the total allowable acute or post-acute expenditures for an episode of care are predetermined. Participants share in losses or savings resulting from the difference between the target price and actual cost for episodes, including costs that result from complications and hospital readmissions.
Bundled payments models, also known as episode-based payment models, are designed to move toward value-based care, incentivizing providers to advance efficiency and coordination of care while also improving patient outcomes at lower costs.
What Are Advanced APMs?
Advanced Alternative Payment Models (APMs) are a type of APM that meets the legislative definition, which states that 50% of participants must use certified electronic health record technology (CEHRT), payments must be based on quality measures comparable to quality measures in the Merit-Based Incentive Payment System (MIPS), and the entity must bear more than nominal financial risk (or is a CMMI Medical Home Model expanded by the secretary of Health and Human Services).
What Is Nominal Risk?
Nominal risk is a condition that must be met by Advanced Alternative Payment Models (APMs) under the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA), which states that Advanced APMs must assume nominal risk, or risk of an amount that is lower than optimal but substantial enough to drive performance.
What Is the Comprehensive Primary Care Plus (CPC+)?
Comprehensive Primary Care Plus, or CPC+, is designated by CMS as an Advanced Alternative Payment Model (APM). CPC+ includes two primary care practice tracks with incrementally advanced care delivery requirements and payment options to meet the needs of primary care practices in the United States.
CPC+ provides practices with a learning system and actionable patient-level cost and utilization data feedback to guide decision making. Practices in both tracks make changes in the way they deliver care, based on core Comprehensive Primary Care functions.
What Is the Oncology Care Model (OCM)?
Oncology Care Model (OCM) is a payment model created by the CMS Innovation Center to promote higher quality and better coordinated oncology care while also lowering Medicare cost. There are two types of Oncology Care Models: 1-sided risk and 2-sided risk arrangements. Those that are 2-sided risk arrangements qualify as Advanced APMs.
Under the OCM, physician practices enter into payment arrangements that include financial and performance accountability for episodes of care surrounding chemotherapy administration to cancer patients.
What Is the Comprehensive ESRD Care Model (CEC)?
The Comprehensive ESRD Care (CEC) model is the first accountable care organization (ACO) with a disease-specific focus created by the CMS Innovation Center with the goal of identifying ways to improve quality and coordination of care for Medicare patients with end-stage renal disease (ESRD), while also reducing Medicare cost.
The two CEC tracks include the Large Dialysis Organization (LDO) arrangement and the non-LDO arrangement. Only the LDO arrangement qualifies as an Advanced APM. The non-LDO does not qualify because it does not bear financial risk.
What Is an ESRD Seamless Care Organization (ESCO)?
An ESRD Seamless Care Organization (ESCO) is an ACO consisting of providers and suppliers who voluntarily unite in a legal entity that offers coordinated care to end-stage renal disease (ESRD) beneficiaries through the Comprehensive ESRD Care (CEC) model.
An ESCO is required to have participant owners that include at least one nephrologist or nephrology group practice and at least one dialysis facility.
What Is the Center for Medicare and Medicaid Innovation (CMMI)?
The Center for Medicare and Medicaid Innovation (CMMI) was created as part of the Affordable Care Act (ACA) to test payment and service delivery models to reduce program expenditures while preserving or enhancing the quality of care. This federal agency oversees programs such as MSSP, TCPI, and ACOs.
Innovation models are organized into seven categories: Accountable Care Organizations (ACOs), episode-based payment initiatives, primary care transformation, initiatives focused on Medicaid and the Children’s Health Insurance Program (CHIP) population, initiatives focused on Medicare and Medicaid enrollees, initiatives to accelerate the development and testing of new payment and service delivery models, and initiatives to speed the adoption of best practices.
What Is an Accountable Care Organization?
Accountable care organizations (ACOs) are groups of doctors, hospitals, and clinicians who voluntarily unite to provide coordinated, high quality care to Medicare beneficiaries with the goal of ensuring patients receive the right care at the right time, while also guarding against needless duplication of services and avoidable medical errors.
When an ACO succeeds in delivering high-quality care and reducing healthcare costs, it shares in the savings it achieves for the Medicare program.
What Is a Next Generation ACO?
The Next Generation Accountable Care Organization (ACO) is designated by CMS as an Advanced Alternative Payment Model (AAPM).
Building on the Pioneer model, a Next Generation ACO sets predictable financial targets and better opportunities to coordinate care with the goal of testing whether strong financial incentives for the ACO, along with better patient engagement and care management, can improve outcomes and lower patient costs.
What Is a Medicare Shared Savings Program?
The Medicare Shared Savings Program (MSSP) is a Congress-created program to facilitate coordination and cooperation among clinicians to improve the quality of care for Medicare fee-for-service (FFS) beneficiaries while also reducing unnecessary costs.
Eligible clinicians, hospitals, and suppliers may participate in the MSSP by establishing or joining an accountable care organization (ACO). The MSSP rewards ACOs that lower their growth in healthcare costs and meet performance standards on high quality, patient-first care. Participation in an ACO is voluntary. CMS has designated MSSP Tracks 2 and 3 as Advanced APMs, or AAPMs.
What Is the Medicare ACO Track 1 Plus?
The Medicare Accountable Care Organization Track 1 Plus (ACO Track 1+) is based on the Medicare Shared Savings Program (MSSP) and designated by CMS as an Advanced Alternative Payment Model, or AAPM. ACO Track 1+ incorporates less risk, or limited risk, compared to the MSSP Tracks 2 and 3.

MACRA Proficiency Course
Are you up to speed on MACRA 2022 requirements? Get your annual MACRA training from AAPC, the leader in medical coding and healthcare business compliance.
Code faster, more confidently, and accurately — every time
When you code with Codify, you have an all-in-one resource at your fingertips to help you be the best coder you can be.