Cut Short the Dilemma of Using Prolonged Services Codes
Are you confident with handling the reporting of prolonged care services? Have you mastered the art of using the new and revised codes correctly? It all boils down to having an eye for detail.
“New prolonged care code for the staff should not be reported for every time the staff spends time with the patient,” says Carol Pohlig, BSN, RN, CPC, ACS, senior coding and education specialist at the Hospital of the University of Pennsylvania. “Medical necessity is the overarching factor.”
Here is a quick brief to help you claim all your deserved reimbursement for your extra hard work on the patients.
Know the Prolonged Service Code Essentials
You need to memorize the basic facts associated with coding prolonged care, such as:
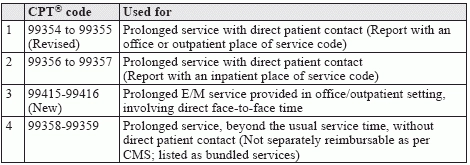
Keeping those guidelines in mind, here are the prolonged service codes that you need to be aware of. CMS reimburses prolonged services with direct patient contact, as add-on codes with the appropriate E/M codes, when the service time is a crucial factor in determining the level of service.
Get Paid For 99354 and 99355
“CPT® codes 99354 and 99355 were designed to separate direct patient contact from time spent coordinating patient care, prior to or following a patient encounter,” says Anthem Blue Cross and Blue Shield’s commercial professional reimbursement policy.
The revised code +99354 stands for Prolonged evaluation and management or psychotherapy service(s) (beyond the typical service time of the primary procedure) in the office or other outpatient setting requiring direct patient contact beyond the usual service; first hour (List separately in addition to code for office or other outpatient Evaluation and Management or psychotherapy service).
The 2016 revision of the official descriptor specifies that the prolonged service is beyond the typical service time of the procedure, and directs you to list separately any other E/M or psychotherapy service. However, the prolonged service time need not be continuous or in a single stretch, as long as the time was spent on the same date of service.
Remember to team it up: With +99354 being an add-on code, remember to report it with the appropriate primary E/M codes such as 90837, 00241-99245, 99201-99215, 99324-99337, or 99341-99350. You should not report 99354 with 99415 or 99416.
To account for the additional minutes of service over and above the first hour, use requisite number of 30-minute units of +99355. For observation and inpatient prolonged services, you may go for +99356 or +99357.
Decipher 99355: CPT® code +99355 represents each additional 30 minutes of prolonged E/M service beyond the first hour of additional time (… each additional 30 minutes [List separately in addition to code for prolonged service]). It can apply to either an office or outpatient E/M or psychotherapy service.
You report +99355 along with +99354; however, remember to not use it with 99415 or 99416.
Plus: Your provider must have spent half of the time listed with the prolonged service code before you can report +99355. For example, if the provider claims she spent a total of 75 extra minutes over and above the typical E/M service times, you may report +99354 for the first hour of prolonged service, and +99355 for the leftover 15 minutes of prolonged service.
According to Anthem, prolonged services may be eligible for separate reimbursement in a few urgent situations such as respiratory distress, severe wheezing, or a severe allergic reaction with swelling. The management here would definitely entail a significant amount of provider time to monitor the patient’s response to treatment. This would be beyond the typical E/M service.
Ace the New Codes for Clinical Staff’s Prolonged Service
The addition of two new codes for 2016 (+99415 and +99416) is a big change to how you’ve reported services in the past. These two exclusively outpatient codes help you report prolonged services time of clinical staff under the supervision of a qualified healthcare professional.
“This is a way to capture some of the educational services that nurses provide which were formerly incorporated into the physician service without being able to bill separately for the staff’s time,” explains Pohlig.
CPT® code +99415 (Prolonged clinical staff service [the service beyond the typical service time] during an evaluation and management service in the office or outpatient setting, direct patient contact with physician supervision; first hour [List separately in addition to code for outpatient Evaluation and Management service]) stands for the first hour of extra time that the clinical staff works (under the provider’s supervision) directly with the patient during an outpatient or office E/M service. Again, you will need to report this add-on code with an appropriate primary code for E/M service.
The other new CPT® code +99416 (… each additional 30 minutes [List separately in addition to code for prolonged service]) is an add-on code you can use to report each half-hour of additional time, beyond the first hour of prolonged services, when clinical staff works directly with the patient during an office or outpatient E/M service.
Remember: You need to use +99416 in conjunction with +99415. First, apply an appropriate base primary code, then include +99415 and +99416 as appropriate. Base primary codes that you can potentially submit with +99415 or +99416, depending on the service provided include: 99201, 99202, 99203, 99204, 99205, 99211, 99212, 99213, 99214, and 99215. However, do not report +99415 or +99416 with 99354 or 99355.
Heed the OIG Radar on Prolonged Services
In the 2016 Office of Inspector General (OIG) work plan, there is a mention of the OIG aiming to explore the reasonableness of prolonged care services. OIG considers the necessity of prolonged services as “rare and unusual.” To counter this, you will need foolproof documentation when reporting prolonged services, specifically containing the following:
The final takeaway: “It is best for the physician to indicate the need for the extended service in his/her plan of care (e.g., patient requires education on prevention of asthma triggers), and the details of the prolonged care session should be documented in the staff note,” contemplates Pohlig. “The time criterion for the physician’s service must be met, regardless of counseling time, before considering to report the prolonged care codes. Once the physician has met his/her time criterion, the staff will then need to account for a minimum of 45 minutes to be able to report 99415. The physician or the staff member should indicate that the physician was available for supervision (i.e., in the office suite, not the patient room).”