Tread Cautiously With the New LDCT Lung Cancer Screening SDM Reporting
ATS approaches requirements critically, asks CMS two questions.
Is your staff aware of the eligibility requirements for Medicare coverage of the lung cancer screening with low dose computed tomography (LDCT)? Empowered by the Social Security Act, which allows CMS to add coverage to services using “additional preventive coverage”- by routing it through the NCD process; CMS now provides coverage for lung cancer with LDCT. Explore with us the factors, requirements, and the issues that come along with this new coverage.
How to Get Started With the Lung Cancer Screening
Medicare seems to be very particular about the sequence of events and the requisite documentation in the process. First of all, the patient undergoes a screening and counseling session, where, if the provider decides the patient requires and is eligible for lung cancer screening with LDCT, he gives a written order for the same.
The visit must include the following components which should be documented in adequate detail.
Shared decision making: The provider must involve the patient in a shared decision making process, explaining the risks versus benefits of the procedure (including exposure to radiation and the possibility of over diagnosis) as well as details regarding further subsequent diagnostic investigations that may be required down the road.
Counseling for the LDCT procedure: The provider explains the significance of regular annual LDCT lung cancer screenings, and how co-morbidities or other illnesses may affect the lung status. He also discusses with the patient his willingness to undergo the arduous process of diagnosis and treatment.
Counseling on smoking cessation: The provider tries to make the patient realize the importance of staying away from tobacco, whether he is a past or present smoker. The provider further helps the patient with information on tobacco cessation interventions.
Who orders the screening? According to an MLN article, only primary care providers can order the above screening and shared decision making visit and counseling.
According to Carol Pohlig, BSN, RN, CPC, ACS, senior coding and education specialist at the Hospital of the University of Pennsylvania, “the original Decision Memo identifies that this would be ‘furnished by a physician (as defined in Section 1861(r)(1) of the Social Security Act) or qualified non-physician practitioner (meaning a physician assistant, nurse practitioner, or clinical nurse specialist as defined in §1861[aa][5] of the Social Security Act).’”
Background
Effective for service claims dating Feb. 5, 2015, onwards, Medicare now covers lung cancer screenings for patients using LDCT who:
-Are between ages 55-77
What this means: Subsequently, CMS has clarified to American Thoracic Society (ATS). In its newsletter Coding and Billing Quarterly, Feb. 2016 issue, ATS states, “the clarification policy provides ample guidance from CMS that all physicians are able to order lung cancer screening and provide the shared decision making service, provided all other CMS criteria are met.” ATS has also reached out to numerous Medicare Administrative Contractors (MACs) to ensure consistency on this issue. The MACs state that they plan to pay claims in this regard from all physician providers, including specialists. Pohlig further informs that “the CMS statement issued to ATS confirming that all physician specialties can furnish this service is available on the ATS website.”
To read the statement, visit http://news.thoracic.org/cms-issues-clarification-on-ldct-lung-cancer-screening-program.
Get Your New G Codes on SDM Visit Right
You now have two new HCPCS codes for the shared decision making (SDM) visit and screening. Here is how you can go ahead and report them:
Patient copays or deductibles are not applicable for these preventive codes. Furthermore, these encounters cannot take place during a phone conversation – they need to be face-to-face encounters.
Written Order Components
-Patient’s date of birth
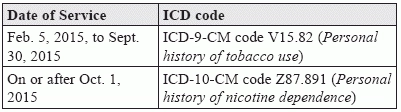
Correct diagnosis code: Although Medicare is providing coverage for lung cancer screenings using LDCT retrospectively to February 2015, it will deny the G0296 and G0297 claims that do not contain time appropriate ICD codes. That means you need to include V15.82 (Personal history of tobacco use) for claims prior to Oct.1, 2015, and Z87.891 (Personal history of nicotine dependence) for claims with a date of service on or after Oct. 1, 2015.
Hold some claims: ATS has questions about the provision for coding for patients who are current smokers, and is in contact with CMS about possibly adding another code, F17.2 (Nicotine dependence), in the future. According to the ATS newsletter, “for those patients who are current smokers, those claims will need to be held, as contractors do not currently have instructions and these claims will be denied.”
Final takeaway: “Ensure that documentation is inclusive of all the required elements for reporting these services,” reiterates Pohlig. “Using a templated note will assist in capturing the detail, and ensure eligibility criteria of beneficiaries. When new services are reported, it is not long before the payers request to review documentation to ensure adequacy of services.”
Expect to read more regarding the institutional billing requirements and the claim adjustment reason codes in the next issue of Pulmonology Coding Alert.
-Do not depict any signs or symptoms of cancer, apparently asymptomatic
-Confirm a smoking history of at least 30 pack years (one pack year means twenty cigarettes smoked every day for one year)
-Might have quit smoking within the last 15 years, or may be smoking presently
-Have a written order for LDCT enabled lung cancer screening, fulfilling the eligibility requirement as per the NCD 210.14.
-Number of pack years
-Smoking status past/present
-Affirmation of patient bring asymptomatic at the time of visit
-NPI of the practitioner