Code for Pressure Ulcers in 4 Easy Steps

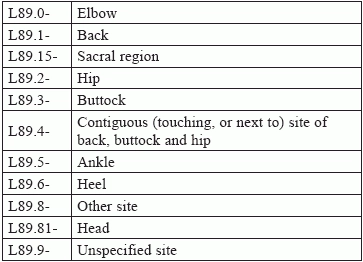
Take this tour through the L89 codes to find bed sore coding relief. Pressure ulcers - or bed sores, as they are more often known - are a common condition affecting many patients who are confined to a bed, chair, or wheelchair for prolonged periods of time. The pressure this exerts on the areas of skin that cover the bones, especially in the back, buttocks, heels, hips, and elbows, causes the skin tissue to become sore and eventually break down. Coding the condition requires coders to pay close attention to ICD-10 conventions regarding sequencing and laterality as well as knowing some specific medical terminology. Following these four simple steps will lead you through the code choice to arrive at the most precise diagnosis code possible. Step 1: Code First for Associated Gangrene If your provider's notes indicate the patient has gangrene, you'll need to code that first before you dig into the L89 codes. ICD-10 directs you to code the condition with I96 (Gangrene, not elsewhere classified) and sequence it before the specified pressure ulcer. Step 2: Code for Site ICD-10 breaks down pressure ulcer sites in the following way. Very often, patients will present with pressure ulcers in multiple sites, which can result in a sequencing issue. When that occurs, go back through your doctor's notes to see, first, if all the ulcers are being treated. If there's only one, then that's all you'll need to code; if there are more, you would sequence them by severity, putting the most severe first. Coders should also be aware that coding L89.89- (Pressure ulcer of other site) is not the same as coding L89.9- (Pressure ulcer of unspecified site). As Melanie Witt, RN, CPC, MA, an independent coding expert based in Guadalupita, New Mexico, explains it, "'Other site' means that the provider has indicated where the ulcer is, but there is no specific code under L89.- that specifies the site documented." "L89.9-," Witt continues, "would mean that the provider has not documented where the ulcer is at all." Coding caution: Marcella Bucknam, CPC, CCS-P, COC, CCS, CPC-P, CPC-I, CCC, COBGC, manager of clinical compliance with PeaceHealth in Vancouver, Washington, warns coders that coding L89.9- "is very rare, but use of the unlisted code is on the rise because physicians have the unspecified code as their default code choice in their EHR [electronic health records]. Using this code," Bucknam advises, "could cause problems for treatment and care reimbursement, as certain care is more appropriate for feet as opposed to the sacrum, hips, or other locations that pressure ulcers may appear." Step 3: Code for Laterality The L89 codes are broken down further by laterality, which means that you can choose between right, left, and unspecified anatomic areas of most sites. There are no bilateral codes, however, which means that pressure ulcers that equally affect both sides of regions such as the hips and buttocks have to be coded separately using the codes for right and left. Step 4: Code for Severity Pressure ulcers are categorized by degrees of severity, known as stages, that correlate to the depth of the tissue damage. They range from stage one, where the skin is merely inflamed and red, through to stage four, where there is bone-deep tissue loss along with necrosis. Here, again, coders can be confused by word use, as ICD-10 classifies two other stages as "unspecified" and "unstageable." In this case, unstageable simply means that the depth, or stage, of the wound cannot be determined as slough and/or eschar are covering the would bed. As both enable the wound to heal, your provider won't remove them to determine the stage, so the stage is classified unstageable. However, Bucknam again warns that coding a pressure ulcer as unstageable is a rare occurrence. Go above and beyond: For more details about the National Pressure Ulcer Staging System, go to https://www.ncbi.nlm.nih.gov/books/NBK2650/pdf/Bookshelf_NBK2650.pdf. A Final Word of Caution Both Witt and Bucknam remind coders to keep a close eye on the documentation they are reviewing. "Pressure ulcer details, like staging," Bucknam says, "are often documented by nurses, and coders should only use documentation provided by the physician." Witt agrees, adding that even though nurse documentation "can be used to code the stage at this encounter, it is the provider who is attending the patient at this visit who is responsible for assigning the severity of the ulcer."