Spot These Easy-to-Miss Bundling Changes, Implemented July 1

Stent placement and fluoroscopy updates could affect your claims.
The medically unlikely edits (see page xxx) aren’t the only changes that will impact your code bundles effective July 1. In addition, CCI has some additional edits in store for your practice.
The July 1, 2014 CCI version 20.2 update brings 20,729 new edit pairs. “With only 212 terminations, we see a net gain this quarter of 20,517 new edit pairs for a total of 1,334,994 active edit pairs (or reasons not to pay you for what you do) in the database,” says Frank Cohen, MPA, MBB, principal and senior analyst for The Frank Cohen Group in Clearwater, Fla.
Know the Cardiology Edits
“Swap” is the name of the game for cardiology edits in CCI 20.2. In a few edits, codes swap columns, and in some other edits you’ll see modifier indicators flip. Here are the details.
Don’t Stop at the Deletions for 37236-+37239
The first set of affected codes involves transcatheter intravascular stent placement codes 37236-37239:
The above codes had the following edits in version 20.1, which became effective in January at the same time that the codes became effective:
Version 20.2 deletes all of the above edits retroactive to Jan. 1, 2014, according to the analysis by Frank Cohen of the healthcare analytics firm The Frank Cohen Group.
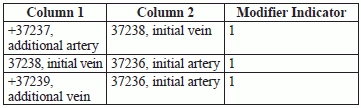
But there’s a catch. Version 20.2 adds back two new edits for these codes:
Bottom line: The modifier indicator of 1 means that you may override the edit with a modifier when appropriate. Specifically, to report additional vein code +37239 on the same date as initial artery code 37236, you’ll need to append a modifier to +37239. You’ll also need to report initial vein code 37238 as the primary code for +37239.
Similarly, to report additional artery code +37237 on the same date as initial vein code 37238, you’ll need to append a modifier to +37237. You’ll also need to report initial artery code 37236 as the primary code for +37237.
Tie to the past: As explained in Cardiology Coding Alert, vol. 17, no. 3, the above changes aren’t the only ones CCI has made to edits for these codes. Version 20.1 retroactively deleted edits preventing you from reporting 37236 with +37237 and 37238 with +37239.
Code 37236 is the only appropriate primary code for add-on code +37237, so an edit that prevents payment of 37236 when reported with +37237 is illogical. The same reasoning applies to the 37238/+37239 edit. As Marchelle Cagle, CPC, CPC-I, PCS, of Cagle Medical Consulting, explained, you should not need a modifier to report an add-on code with its primary code, so deleting these edits made sense.
Don’t Abuse Fluoro Modifier Indicator Switch
Another swap you’ll see in version 20.2 is the modifier indicator for many edits with column 2 code 76000 (Fluoroscopy [separate procedure], up to 1 hour physician or other qualified health care professional time, other than 71023 or 71034 [e.g., cardiac fluoroscopy]).
The modifier indicator switches from 0 to 1, meaning that you will now be able to report 76000 with a modifier on the same date as the column 1 procedure, but only if the fluoroscopy is a distinct service.
The relevant column 1 codes you should note are as follows:
Bottom line: Just because CCI allows you to override an edit, that doesn’t mean you should override the edit. Only override the edit when documentation clearly shows the use of fluoroscopy was truly distinct from the column 1 procedure.
Surgical Coders: Resist Separate Vessel Repair
If your surgeon performs procedures in a provider based clinic (also called a provider based entity, or PBE), meaning that the hospital owns the clinic, you might have some concerns when billing 99201-99215 (Office or other outpatient visit for the evaluation and management of a … patient…). That’s because, this year, CMS collapsed that 10-code sequence into a single code that the hospital bills for outpatient payment: G0463 (Hospital outpatient clinic visit for assessment and management of a patient).
Now CMS adds more than 5000 edit pairs for G0463 (Hospital outpatient clinic visit for assessment and management of a patient) with surgical procedures.
Do this: If your surgeon performs an unrelated evaluation and management service for a hospital outpatient at a PBE, you’ll continue to bill the appropriate code from the range 99201-99215. But the hospital billing for the service would need to check whether the procedure is bundled with G0463 before reporting that code.
Caveat: These CCI edits won’t apply if you’re billing for your surgeon’s services in most physician offices (place-of-service 11).
Avoid Separate Blood Vessel Repair Codes
When your surgeon performs any of a number of vascular procedures, such as injection or catheter placement codes in the range 36005-37500, or balloon angioplasty codes in the range 35450-35476, you’ll be facing new CCI 20.2 edit pairs with the following blood vessel repair codes in the column 2 position:
“These bundles make sense if the two procedures, such as catheter placement and blood vessel repair, involve the same vessel,” says Marcella Bucknam, CPC, CPC-I, CCS-P, CPC-H, CCS, CPC-P, COBGC, CCC, internal audit manager with PeaceHealth in Vancouver, Wash. “But if the two procedures involve distinct services on different vessels, the CCI modifier indicator of ‘1’ allows you to bill both services with a modifier such as 59 (Distinct procedural service),” she says.
Learn Other Surgical Bundles
CCI 20.2 holds many more edit pairs that you need to know about for your general surgery practice.
For instance, there are new edit pairs for 17000 and 17004 (Destruction [e.g., laser surgery, electrosurgery, cryosurgery, chemosurgery, surgical curettement], premalignant lesions [e.g., actinic keratosis] …) as column 1 codes with many of the following codes:
If your surgeon performs the bundled procedures on different lesions at different sites, you can use modifier 59 to override the edit pairs.
Don’t break these bundles: You might need to be aware of new edit pairs with the following HCPCS Level II codes for hospital billing if your surgeon performs the services at a PBE. CCI 20.2 lists these with a modifier indicator of “0,” meaning that you can’t override the edit pairs under any circumstances.
Specifically, CCI 20.2 creates edit pairs for skin substitute graft codes C5271-C5278 with 15271-15278 (Application of skin substitute graft to …). Due to large variations in cost for skin substitute materials, Medicare instituted a two-tier coding system for skin substitute graft application beginning Jan. 1, 2014. Codes C5271-C5278 are for procedures using low-cost materials, and 15271-15278 are for procedures using high-cost materials. The material classification as low- or high-cost is based on CMS’s designation, which you can find in MLN Matters Number MM8572.
Anoscopy edits: If your surgeon performs pretty much any procedure involving rectum, anus, or colon in the code range 45000-46947, you’ll find the procedure bundled with C9735 (Anoscopy; with directed submucosal injection[s], any substance) for hospital billing.