
ICD-10: See How 'Medical Necessity' Factors into GI Surgery Pay

Tip: Pinpoint coding to correspond with symptoms and final diagnoses. With a plethora of diagnosis codes available, coders can truly differentiate between various conditions for gastrointestinal surgery claims. This myriad of options can also significantly boost your practice's procedure pay. Because the surgeon or the referring clinician may describe symptoms that are the indication for surgery, you'll need to be able to "decode" any narrative diagnoses you receive, and report the best ICD-10 code. Remember: You should wait for the pathology report, when possible, and list the final diagnosis on the claim. Without that information, you'll need to report the signs and symptoms that the surgeon or referring clinician initially reported. Never: Don't report an undiagnosed condition that the surgeon or clinician noted as "rule out" or "suspected." You can clip and save the following chart for a quick reference tool for common GI diagnoses. Also read on for expert tips about using these codes. Distinguish Symptoms from Definitive Dx Reporting GI diagnoses may involve coding symptoms or conditions. "Whether you gravitate to the R or K sections [of ICD-10] depends on whether you're coding signs and symptoms (R) or a definitive diagnosis (K)," says Kent Moore, senior strategist for physician payment at the American Academy of Family Physicians This will help you make the correct choice between two codes that appear to be the same. For example, Moore explains that "R19.7 [Diarrhea, unspecified] represents a sign or symptom of some other underlying condition, which the physician may or may not have diagnosed yet. In comparison," Moore goes on, "K59.1 [Functional diarrhea] represents a definitive diagnosis of a functional intestinal disorder. Basically, the person has diarrhea because his or her bowels don't function properly, not because of some other underlying cause like food poisoning or a virus, for example." Another example: You should code heartburn R12 (Heartburn) "if the condition is not considered to be chronic and does not show the various symptoms of GERD," says Chelle Johnson, CPMA, CPC, CPCO, CPPM, CEMC, AAPC Fellow, billing/credentialing/auditing/coding coordinator at County of Stanislaus Health Services Agency in Modesto, California. But "GERD can have additional symptoms, such as heartburn, chronic cough, difficulty swallowing, and in some cases laryngitis," Johnson says, in which case you should turn to K21.- (Gastro-esophageal reflux disease). Distinguish Hernia Codes with 3 Questions Hernia repair may be a general surgeon's bread and butter, so you need to know more than the chart shows to choose the right diagnosis out of nearly 45 codes in the range K40-K46. As you read the surgical note, ask yourself these questions to help you zero in on the right code: Question 1: What type of hernia is this? ICD-10 breaks it down into the following basic types: Question 2: Is the hernia reducible or strangulated, or causing an obstruction? Remember these terms: Question 3: Does the op note mention gangrene? Tissuedeath of the hernia leads to a different code choice than a hernia that does not involve gangrene, such as K44.0 (Diaphragmatic hernia with obstruction, without gangrene) versus K44.1 (Diaphragmatic hernia with gangrene). Question 4: Do you see any information about laterality or recurrence in the op note? Some of the hernia codes distinguish unilateral versus bilateral hernias, and whether the condition is recurrent, such as K41.90 (Unilateral femoral hernia, without obstruction or gangrene, not specified as recurrent) versus K41.91 (Unilateral femoral hernia, without obstruction or gangrene, recurrent) or K41.20 (Bilateral femoral hernia, without obstruction or gangrene, not specified as recurrent).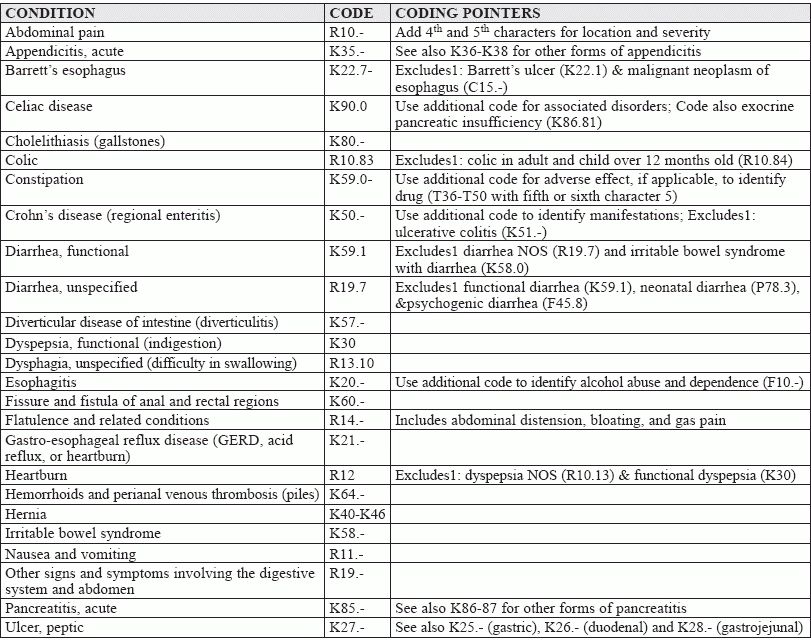
(List adapted from the American College of Gastroenterology http://patients.gi.org/topics/common-gi-symptoms/ and the American Academy of Family Physicians www.aafp.org/fpm/2015/0100/p19.html)



