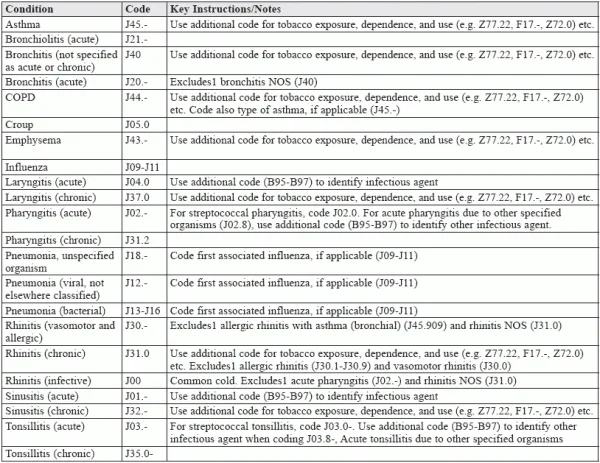
Simplify Your Respiratory Dx Coding with this Comprehensive Chart
Plus, incorporate this expert advice into your Coding respiratory diagnoses is notoriously challenging for ENT coders for good reason. The codes are heavily nuanced and include enough instructional notation to trip up even the most experienced coders. That’s why we’ve prepared for you this helpful reference page to fall back on when respiratory coding leaves you feeling short of breath. If that’s not enough, take a look at these key pointers to help you report J codes with confidence and precision. Expert Tip 1: Pinpoint Cause for Precise Pneumonia Coding To make life difficult for coders, “there are about 75 codes in ICD-10-CM to describe various forms and causes of pneumonia in adults,” says Melanie Witt, RN, CPC, MA, an independent coding expert based in Guadalupita, New Mexico, “and another 13 in children after birth.” “Coding for pneumonia will rely on the organism that has been confirmed as the cause or the combination disease the patient may have with the pneumonia,” Witt continues, adding that “even though there are some codes that can be reported when the type of organism is not known, if a sputum test or culture has been performed, you should have this information at hand and select the most accurate code.” Expert Tip 2: Know the Difference Between Bronchitis and Bronchiolitis They may sound the same, but “the difference between bronchitis and bronchiolitis is the difference between what part of the lungs are actually infected,” says Marcella Bucknam, CPC, CCS-P, COC, CCS, CPC-P, CPC-I, CCC, COBGC, revenue cycle analyst with Klickitat Valley Health in Goldendale, Washington. As Bucknam puts it, “the bronchioles are the small, delicate airways that lead directly to the alveoli, which are the microscopic cul-de-sacs of the lung tree, whereas the bronchi are the larger pipes that make up the first two to three branches of the lungs immediately after the trachea.” However, advises Bucknam, “even if there is an x-ray that includes that information, a coder cannot make the decision of coding bronchitis versus bronchiolitis unless a provider has documented that diagnosis.” Expert Tip 3: Distinguish Between Viral and Bacterial for Sinusitis As Witt further points out, “distinguishing conditions such as acute viral rhinosinusitis related to colds and influenza-like illnesses from bacterial infection is a frequent challenge, even to the otolaryngology clinician.” So, like pneumonia, it is important to look for the etiology of the sinusitis in the record. But just as coders should not distinguish between bronchitis and bronchiolitis from an x-ray, “they cannot assign a code for, say, frontal sinusitis unless a physician has provided a diagnosis that specifies that disease,” according to Bucknam. “Without a provider’s interpretation,” Bucknam cautions, “the information cannot be used by a coder to assign codes.” The bottom line: “A frequent problem that I’m seeing in current medical record documentation,” Bucknam tells coders, “is that the physician is guided to choose a diagnosis code that has more detail than is documented anywhere in the record.” Consequently, Bucknam suggests, “coders should coach physicians to record as many details as are known. Coders are not qualified to distinguish between diagnoses based only on exam findings or other documentation of symptoms,” Bucknam adds. “That,” Bucknam reminds coders, “is the provider’s sole responsibility.”