Take Note of These Minor E/M Changes for 2024
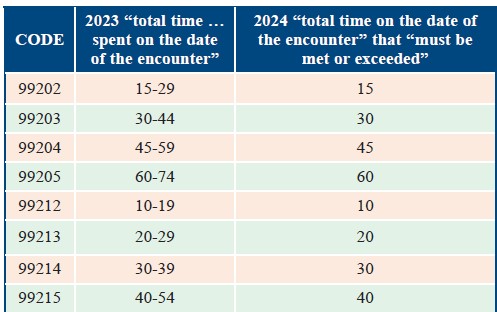
Find out if the modified descriptors will change how the codes are used. The year is coming to a close, which means the AMA’s annual updates to the CPT® code set are about to take effect. Do this year’s 230 additions, 49 deletions, and 70 revisions have you wondering where to begin? Start by studying the revisions to the evaluation and management (E/M) codes and how they may impact documentation and coding practices once the calendar flips to Jan. 1, 2024. Read on for a breakdown of the changes on the horizon to ensure you’re on the path to coding success. See What Replaced Time Ranges in Revised Descriptors The 2024 E/M changes are minimal, but that doesn’t mean they are insignificant. CPT® has decided to remove the time ranges from both the new and established office/outpatient E/M codes and replace them with a single total time amount, which is the lowest number of minutes in the current range for each code. This time “must be met or exceeded” according to the new wording that appears in each of the codes’ descriptors. Examine the descriptor differences between 2023 and 2024 below: For example, 99202 (Office or other outpatient visit for the evaluation and management of a new patient, which requires a medically appropriate history and/ or examination and straightforward medical decision making …) has a current time range of 15-29 minutes. However, beginning Jan. 1, 2024, the provider must meet or exceed 15 minutes of total service time on the date of the encounter for time-based coding, as indicated by the revised code descriptor: (… When using total time on the date of the encounter for code selection, 15 minutes must be met or exceeded.). Why: The changes make the office codes more “consistent with the language of the other timed E/M codes,” explains Melanie Witt, RN, MA, CPC, an independent coding expert based in Guadalupita, New Mexico. In table form, the changes look like this: Key: “This doesn’t really change how the codes are used, but listing the minimum time instead of a range for each code is probably going to be easier to follow,” says Kelly Loya, CPC, CHC, CPhT, CRMA, CHIAP, associate partner at Pinnacle Enterprise Risk Consulting Services. The AMA’s decision to change the office/outpatient E/M time requirements from a range to a minimum number of minutes reflects Medicare policy. “This revision safeguards providers from using CPT® language that is inconsistent with Medicare policy. Medicare does not permit time ranges to be documented for certain services and wants a specific amount (e.g., integer) of time identified in the documentation,” says Carol Pohlig, BSN, RN, CPC, manager of coding and education in the department of medicine at the Hospital of the University of Pennsylvania in Philadelphia. Watch for Prolonged Service Resolution One possible result of the E/M office/outpatient code changes may be the resolution to the dispute between CPT® and the Centers for Medicare & Medicaid Services (CMS) over the prolonged service threshold times. Remember: CPT® instruction states that prolonged services begin at the minimum time for 99205/99215, while CMS states that prolonged services begin beyond the maximum time. For that reason, CMS created a distinct code, G2212 (Prolonged office or other outpatient evaluation and management service(s) beyond the maximum required time of the primary procedure …) for reporting prolonged services to Medicare. “CMS sought clarifications on the reporting of E/M services, which prompted revisions to the CPT® 2024 code set, specifically revisions to remove time ranges from office or other outpatient visit codes,” says Robin Peterson, CPC, CPMA, manager of professional coding and compliance services, Pinnacle Enterprise Risk Consulting Services, LLC in Centennial, Colorado. Possibility: Now that the time ranges for 99205/99215 have been replaced by a threshold at the minimum end of the range, it is possible that Medicare may follow CPT® rules and adopt +99417 (Prolonged outpatient evaluation and management service(s) time … each 15 minutes …) for prolonged services instead of G2212. Stay tuned to Ophthalmology and Optometry Coding Alert for further information. Keep Up With Other E/M Nuances In light of the changes, you should also recall some basic principles about using the office/outpatient E/M codes. For instance: “Total time will still include face-to-face time as well as time the physician and/or qualified healthcare professional (QHP) personally spent on the patient’s care on the day of the encounter,” explained Jacob Swartzwelder, CPC, CRC, CIC, CEMC, AAPC Approved Instructor, managing director at Compliant Approach Partners, LLC in Las Vegas, Nevada during his HEALTHCON Regional 2023 presentation. “But it doesn’t include time spent in the performance of separately reported services,” he said. 99211: CPT® 2024 does not change the descriptor to 99211 (Office or other outpatient visit for the evaluation and management of an established patient that may not require the presence of a physician or other qualified health care professional). You should continue to bill 99211 for established patients receiving E/M services from a nurse practitioner (NP), a physician assistant (PA), or any other nonphysician practitioner (NPP). The code will also continue to require no level of medical decision making (MDM) or total time for you to document. Nursing facility: In addition to the outpatient E/M (99202-99215) modifications, CPT® 2024 implements a revision to nursing facility care codes 99306 (Initial nursing facility care, per day, for the evaluation and management of a patient …) and 99307 (Subsequent nursing facility care …), raising their time thresholds by five minutes to 50 and 20 minutes, respectively. “It will be important for providers to know these new, higher thresholds if they are seeing patients in a nursing facility,” Loya notes.