
Boost Coding Accuracy with this Intake Form
When your agency begins to use ICD-10, you’ll need much more specific information from your intake staff to assess, code, bill, and keep your money. “ICD-10 is going to throw a whole new wrench in the spokes of our already wobbly wheel,” says Delaine Henry, COS-C, HCS-D, with Health Care Management and Billing Services in Lafayette, La.
When it comes to gathering good information at intake, a form that prompts clinicians to ask for what you need is invaluable. Try this example from Pat Jump with Rice Lake, Wis.-based Acorn’s End Training & Consulting.
CLIENT PHONE REFERRAL/INTAKE FORM
Inquiry Date__________Referral Date (M0104)_________TIME_______CALLER___________________#________
Inpatient Discharge Date (M1005)_________Agency Staff Taking Referral:__________________________________
Referral Source
Pt. Name_______________________________________BD___/___/____ TEL.#____________________________
Address_________________________________________________________________________________________
Pt. Allergies______________________________Service Request: SN PT SLP OT HHA Homemaker
PAYER(s): Medicare PPS HMO/Medicare Advantage Medicaid Waiver Private Insurance Private Pay
Other ________________________________ Payer Verification Done (by HHA Staff): Yes No _____________
PHYSICIAN-ORDERED SOC (M0102) __________________ Start Of Care (M0030) _______________________
PHYSICIAN FOR POC______________________________TEL.#______________ LIC/NPI ___________________
ADDRESS______________________________________________________________________________________
Specific Orders & Misc. Notes_______________________________________________________________________
_______________________________________________________________________________________________
Was Face-to-Face Encounter Completed: Yes No
Was Depression Screening done? Yes No If yes, results: ________________________________________
Physician-ordered protocols (specify)?________________________________________________________________
Recent History of Falls: Yes No ________________________________________________________________
Immunization status: Influenza vaccination_____________________ Pneumonia vaccination___________________
Pressure Ulcer history (include stages)?_______________________________________________________________
Current Pressure Ulcer Treatment_____________________________________________________________
Equipment Needs: ________________________________________________________________________________
Family Contact Information: ________________________________________________________________________
Client Accepted for Service: Yes No (list reason not accepted) ________________________________________
OASIS WORKSHEET FOR REFERRAL/ADMISSION
M0110 Episode 1 early 2 later UK unknown NA not applicable, no Medicare case mix group to be defined
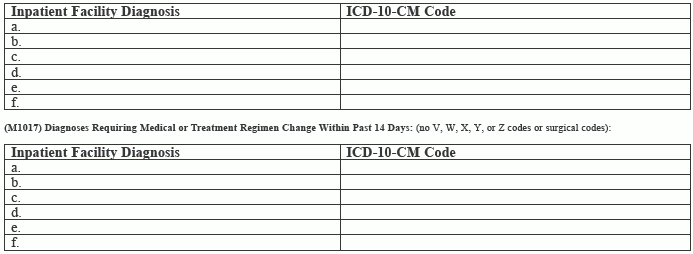
(M1011) List each Inpatient Diagnosis and ICD-10-C M code at the level of highest specificity for only those conditions actively treated during an inpatient stay having a discharge date within the last 14 days (no V, W, X, Y, or Z codes or surgical codes):
M1018 Conditions Prior to Medical or Treatment Regimen Change or Inpatient Stay within past 14 days
1 — Urinary incontinence

2 — Indwelling/suprapubic catheter
3 — Intractable pain
4 — Impaired decision-making
5 — Disruptive or socially inappropriate behavior
6 — Memory loss to the extent that supervision required
7 — None of the above
NA — No inpatient facility discharge and no change in medical or treatment regimen in past 14 days
UK — Unknown
