Follow 6 Steps For Accurate Section Q Coding
Pitfall: Don’t let feasibility issues trip up your coding
When Section Q — Participation in Assessment and Goal Setting triggers a Care Area Assessment (CAA), the RAI Manual requires that you document the discharge plan. And how you code Section Q, care plan for discharges, and ultimately follow through on referrals can greatly impact your survey and certification requirements.
Here are some expert tips to help you accurately — and successfully — complete Section Q:
1. Don’t Always Look for Deficits
First and foremost, understand that not all triggered care areas signal deficits or problems, according to the California Department of Public Health (CDPH). In fact, some care areas may indicate strengths.
Example: Item G0900A — Resident believes he or she is capable of increased independence is an Activities of Daily Living (ADL) area where there is potential for improvement, CDPH says.
2. Make Sure the Resident is Actively Involved — If at All Possible
Whenever possible, the resident must be actively involved in his plan of care, CDPH stresses. The care plan should be “resident-driven and individualized.” Your residents’ involvement in their care affects the dignity and self-determination survey and certification requirements.
Payoff: “Residents who actively participate in the assessment process and in developing their care plan through interview and conversation often experience improved quality of life and higher quality of care based on their needs, goals, and priorities,” CDPH states.
But if the resident is unable to understand the process, you should seek input from the resident’s family members, significant other, and/or guardian or legally authorized representative.
3. Code Even if Resident’s Goals are Unrealistic
Although returning home or discharging to a non-institutional setting could be important to a resident’s health and quality of life, in some cases the resident’s goal may be unlikely or unrealistic, CDPH says. Still, you should code Section Q based on the resident’s expressed goals, even if staff believe those goals aren’t attainable.
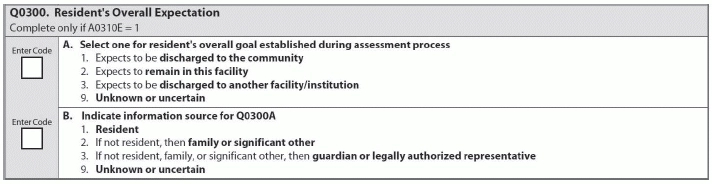
Example: So if Mrs. Smith tells you that she expects to be discharged and return home, even though she does not have proper social support available to do so, you would still code Q0300A — Select one for resident’s overall goal established during assessment process as 1 — Expects to be discharged to the community.
4. Get in Touch with LCA Experts
You should discuss with the resident his interest in talking with Local Contact Agency (LCA) experts about returning to the community, CDPH advises. The LCA can provide various community resources for support in helping the resident to return to a community setting.
If the answer to Q0400A — Is active discharge planning already occurring for the resident to return to the community? is 1 — Yes, then skip to Q0600 — Referral. But if you are not already actively doing discharge planning, code Q0400A as 0 — No, and then move on to code Q0490 — Resident’s Preference to Avoid Being Asked Question Q0500B and Q0500 — Return to Community.
Item Q0500 triggers follow-up actions initiating and maintaining collaboration between your facility and the LCA to support the resident’s expressed interest in transitioning to community living, CDPH notes. You should support the resident in achieving his highest level of functioning, and the LCA should provide the resident with informed choices for community living.
Strategy: Make sure that you ask routine questions of all residents when coding this section, at the initial assessment and in subsequent follow-up assessments, CDPH recommends. If you’re coding 1 — Yes for Q0500B (Do you want to talk to someone about the possibility of leaving this facility and returning to live and receive services in the community?), that signals a request for more information, and you must then contact the LCA about available support in the community.
Caveat: But keep in mind that “answering Yes does not commit the resident to leave the nursing home at a specific time, nor does it ensure the resident will be able to move back to the community,” CDPH points out. And answering 0 — No for Q0500B is not a permanent commitment either. You must inform the resident that he can change his response at any time.
5. Follow the Skip Patterns to Ease Emotional Upset
For some residents and their caregivers, simply bringing up the subject of leaving the facility when it’s not feasible can be upsetting. In these cases (particularly when the resident is cognitively impaired), following the skip patterns in Section Q can give you a big helping hand.
Look at the resident’s record to determine whether he’s indicated in the past that he would like you to ask him about leaving the facility only on comprehensive assessments. If this is the case, then you can code Item Q0490 as 1 — Yes, and skip to Item Q0600. This skip pattern lets you off the hook when you’re completing Section Q as part of a quarterly, correction to quarterly, or non-OBRA assessment (A0310A = 02, 06, 99).
Remember: Although Item Q0490 allows the resident to opt-out of being asked during quarterly assessments about leaving the facility and returning to the community, you still must ask him during the annual comprehensive review, according to the Illinois Department of Healthcare and Family Services.
6. Understand Your Residents’ Community Living Potential
When your resident tells you that he wants to go home, you are probably thinking about all the pros and cons, as well as the practicability, of this decision. According to a recent presentation by Becky Kuhn, statewide MDS Section Q manager for the Ohio Department of Medicaid’s Bureau of Long-Term Services & Supports, you can also look at other factors in the resident’s community living potential, such as:
But if you’ve made the referral by coding Q0600 — Has a referral been made to the Local Contact Agency? as 2 — Yes, referral made, then that trumps everything, Kuhn said.