Boost Your Coding Accuracy With Expert Tips On Resident Interviews
Seek out family members to help with resident interview on daily/activity preferences.
Some of the most vital information you can glean from the MDS is typically from the resident interview sections, especially when you’re care planning. But interviewing residents isn’t always easy, nor is coding the resident interview items. Follow these tips to improve your coding of the resident interviews for cognitive ability, mood, daily and activity preferences, and pain.
Look to B0700 for Ability to Interview
Before you attempt any of the resident interview sections of the MDS, you should first look to the coding of item B0700 — Makes Self Understood to determine whether attempting an interview is feasible. You should attempt to interview all residents unless they’re rarely or never understood, as evidenced by coding item B0700 as 03 — Rarely/never understood.
You must attempt the interviews if B0700 is coded as 0 — Understood, 1 — Usually understood, or even 2 — Sometimes understood.
Important: You must conduct the assessment for B0700 using the resident’s preferred language and consult with staff who care for the resident across all shifts, says Kris Mastrangelo, president and CEO of Harmony Healthcare International. Observe and assess the resident directly, and observe and assess the resident’s interactions with others over all shifts.
Get an interpreter if needed (this includes an American Sign Language interpreter when necessary) and use cue cards, advises Becky LaBarge, RN, RAC-MT, consultant and American Association of Nurse Assessment Coordination (AANAC) Master Teacher. Choose a private, quiet setting to conduct the interviews.
When You Should Stop the BIMS
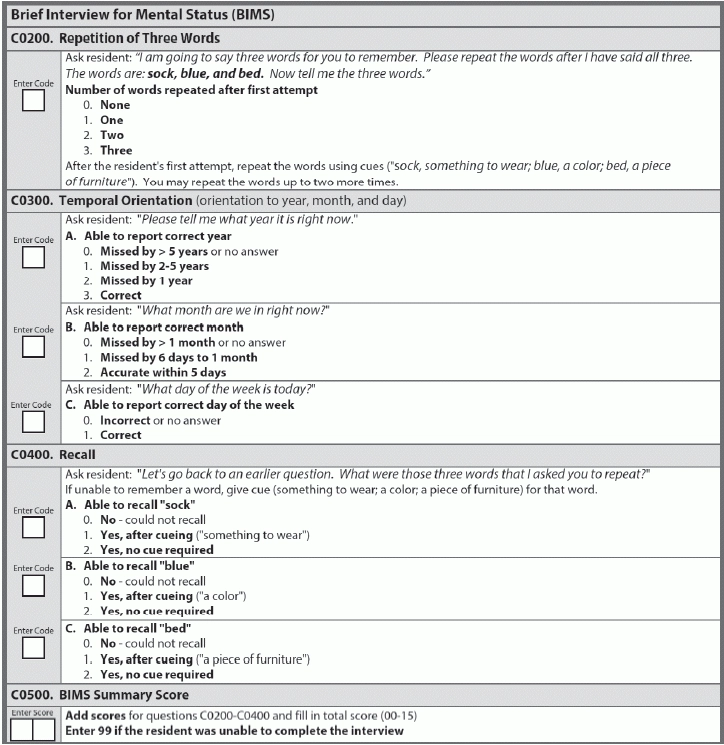
The first resident interview in the MDS is the Brief Interview for Mental Status (BIMS), which is located in Section C — Cognitive Patterns. The rationale for the BIMS is that direct or performance-based testing of cognitive function reduces the chance of incorrect labeling of cognitive ability and improves detection of delirium, LaBarge notes.
To be relevant, the resident’s response only has to be related to the question (logical); it does not have to be correct, Mastrangelo says. You can stop the interview after completing item C0300 — Temporal Orientation if:
The resident must attempt and provide relevant answers to at least four of the questions included in C0200-C0400 for this to be considered a completed interview, Mastrangelo notes.
Know When PHQ-9 Interview is Complete
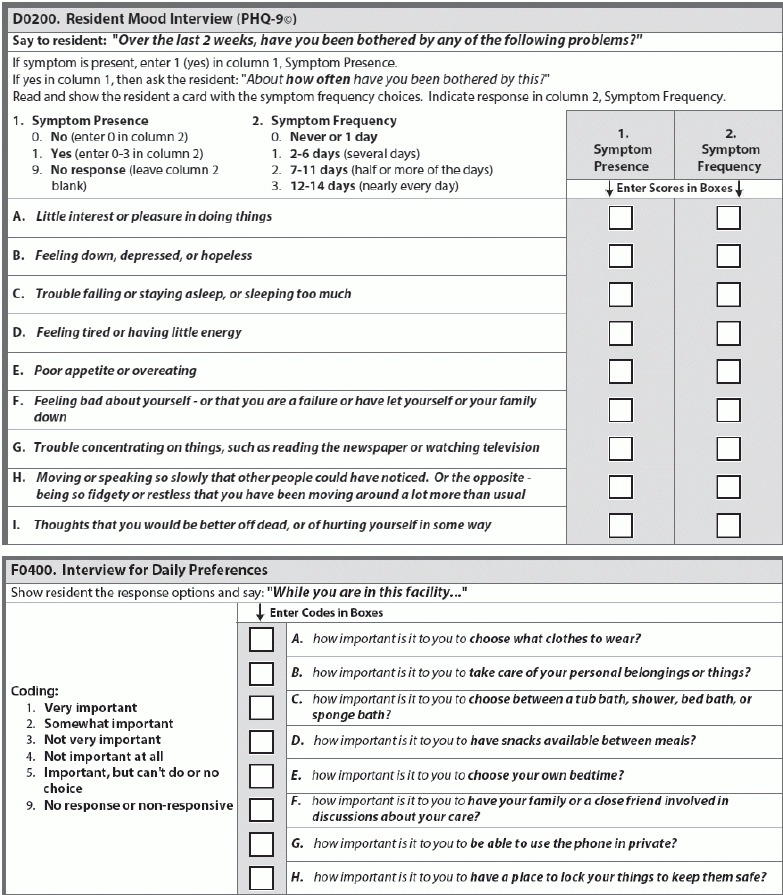
Item D0200 — Resident Mood Interview (PHQ-9©) addresses mood distress, a serious condition that is underdiagnosed and undertreated in the nursing home setting and is associated with significant morbidity, according to LaBarge. “Obtaining information about mood directly from the resident, sometimes called ‘hearing the resident’s voice,’ is more reliable and accurate than observation alone for identifying a mood disorder.”
To be considered a completed interview, the resident must answer the frequency response of at least seven of the nine items in the PHQ-9©, Mastrangelo notes. If the symptom frequency is blank for three or more items, the interview is considered incomplete and you should conduct the staff assessment instead.
Take Advantage of Extra Options for Coding Resident Preferences
Keep in mind that F0400 — Interview for Daily Preferences is the only interview that doesn’t rely solely on patient self-reporting, Mastrangelo says. If a resident is unable or unwilling to participate in the interview, you should conduct the interview with a family member or significant other.
If the resident gives nonsensical responses or fails to respond to three or more of the 16 items in items F0400 and F0500 — Interview for Activity Preferences, the interview is considered incomplete, according to Mastrangelo. If you have to stop the interview because of this, code the remaining questions as 9 — No response or non-responsive, and then proceed with the staff assessment.
Solicit Resident Feedback on Pain
The rationale behind the resident interview for the pain assessment is that any information gleaned directly from the resident about his level of pain is helpful in care planning for pain treatment, Mastrangelo explains. So if the resident is able to provide a relevant answer to J0300 — Pain Presence, you should go ahead and complete the rest of the pain interview.
Strategy: You should conduct this interview close to the end of the five-day lookback period, LaBarge recommends. Preferably, conduct the interview on the day before or the day of the Assessment Reference Date (ARD).
But if the resident is unable to answer J0300, you should skip to the staff assessment for pain, Mastrangelo instructs. And if the resident is unable to answer J0400 — Pain Frequency, code this as 9 — Unable to answer, and then also complete the staff interview.
Bottom line: For all the resident interview sections in the MDS, be sure to follow the script provided. Resident and staff interviews are scripted for a reason, and you should follow the interview scripts exactly, according to Mastrangelo.
“This ensures that there is reliability between different staff members and assures that each overall score is an accurate representation of the patient’s deficits,” Mastrangelo explains. “If the scripted interview process is not followed, variations of the overall score may be representative of different interview techniques, and not changes in the patient’s overall condition.”