
Brush Up On ICD-10 Coding Know-How
Make Section I easier with a basic understanding of how to look up codes. If you’ve ever approached Section I (Active Diagnoses) with trepidation, spending some time getting to know ICD-10 better can simplify your paperwork anxiety. Luckily, the MDS has many of the most common active diagnoses available for easy documentation by simply checking a box. However, if anything else comes up, you’ll need to understand the basic “language” of ICD-10 in order to accurately document the resident’s condition. Understand The ICD-10 Framework Though coding with ICD-10 is tricky, understanding how the codes are organized is the first step to understanding how to manage effective documentation. ICD-10 codes can be up to seven characters, including letters and numbers. Caveat: Some codes are shorter and knowing how many characters a particular code requires is a crucial piece of ensuring successful documentation — and reimbursement. You can think of ICD-10 codes as comprising up to three segments: Category: First three characters (if adding more characters) OR code (if complete) Subcategory: Four to six characters OR code (if complete Code: Seven characters, OR three to six characters (if complete) Though the longest code is seven characters, the MDS boxes for codes have eight spaces. The eight spaces ensure that you have enough room to include a decimal point, which is a necessary organizational bit of many codes. Remember: One crucial aspect of nailing ICD-10 coding is paying meticulous attention to the exact parameters of a situation and diagnosis. For example, if a resident needs a leg amputated due to complications from diabetes, you can’t use the code that signifies amputation due to traumatic injury or poisoning or other external causes. Follow These Rules When you’re trying to figure out which code to use, it’s helpful to know where and how to begin. If you have an ICD-10 Manual or access to an online coding lookup tool, such as TCI’s Codify, you’ll be using the following information as your basic plan to find the correct code: 1. Locate the main term or keyword in the alphabetic index. If you have a manual, take advantage of the color coding to really buoy your understanding of how everything is organized. For example, different categories are visually differentiated with different colors. Although ICD-10 coding is as complicated as it looks, there are some basic rules that hold fast regardless of the code. The first three characters will always follow this format: Letter, Number, Number. As you can see from the chart below, the four remaining characters, when they’re necessary, may be either a letter or a number, depending on the code. The seventh character is one change from the previous coding system, ICD-9. In skilled nursing, you may need a code with a seventh character in order to accurately convey the sequence of encounter, a sequela, or whether the resident’s diagnosis is due to an external cause. In other situations, the seven character can denote birth order, such as in a multiple fetus birth. Pay Attention When you’re looking at a code and deciding whether it’s correct for your resident’s situation, make sure you read everything. There may be pertinent information hiding that could force you to use a different code entirely or point you toward an exclusion you may not have anticipated. Make sure you look for the following notes to ensure you choose the code that most accurately describes your resident’s diagnostic situation: The Excludes1 and Excludes2 notes are sort of self-explanatory and come into play when another code may better apply to your resident’s situation. For example, code S88.011A (Complete traumatic amputation at knee level, right lower leg, initial encounter) has an Excludes1 note: traumatic amputation of ankle and foot (S98.-). Dive into the Nuts and Bolts Using a traumatic leg amputation as an example, the breakdown of the correct ICD-10 code would require the code S88.011A (Complete traumatic amputation at knee level, right lower leg, initial encounter), which would break down as follows: S88 = Traumatic amputation of the lower leg Note: The “initial encounter” part of the descriptor is key. If your resident had a traumatic amputation at knee level on the right leg, but it happened 40 years ago, you wouldn’t use this code. Instead, you would use code Z89- (Acquired absence of limb) and include the pertinent [required] fourth character. It’s important to note the amputation because the residents’ needs may be different, i.e. he may have mobility issues that would affect the planning and delivery of his care while he’s at your facility. 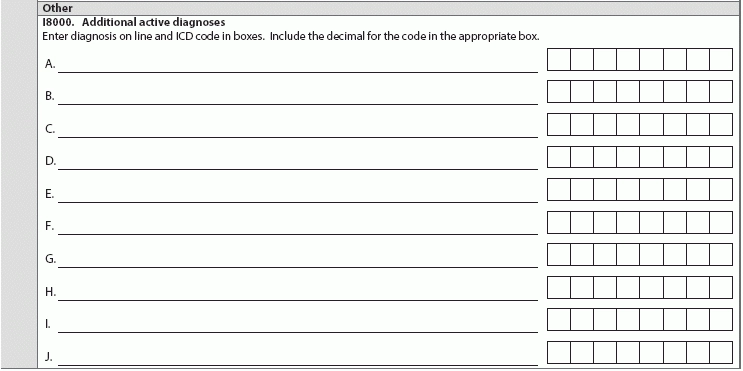
2. Verify the code and identify the highest specificity (i.e., which side of the body, whether this is an initial visit).
3. Review the chapter specific coding guidelines and tabular notes.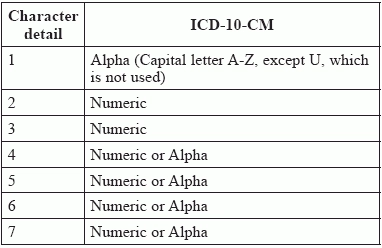
S88.0 = Knee level
S88.01 = Complete amputation
S88.011 = Right lower leg
