Know These Differences Between Attention Disorders

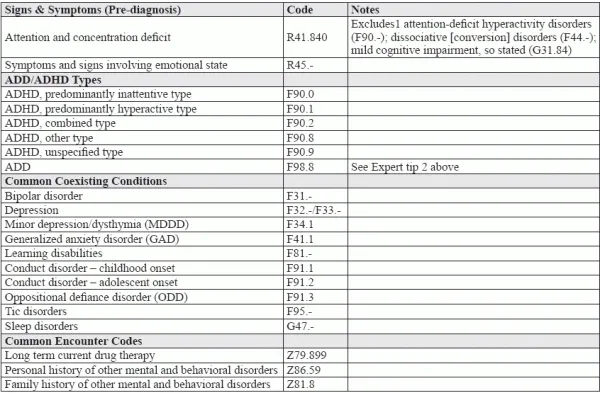
Distinguish these subtleties to ensure accurate coding. Diagnosing and coding attention-deficit disorders may seem easy, but knowing how these distinguishing factors play into the final diagnosis is crucial. Understand these differences between attention-deficit/hyperactivity disorder, or ADHD, and attention-deficit disorder, or ADD, to help eliminate billing issues down the road. Plus, many of your young patients with the conditions will exhibit one or more coexistent condition, so your ability to know and zero in on those conditions quickly and efficiently is key. Clip and save this chart as a handy reference tool to use whenever your pediatrician provides a diagnosis of these mental and behavioral disorders. And we’ve also included three expert tips to help you navigate your code choices with precision. Expert Tip 1: This Associated Procedure Code can be a Clue “If a provider has not yet made the diagnosis of ADHD, some of the codes from the sign/symptoms chapter may be used,” says JoAnne M. Wolf, RHIT, CPC, CEMC, AAPC Fellow, coding manager at Children’s Health Network in Minneapolis, Minnesota. To make the diagnosis, “your provider will probably perform the National Institute for Children’s Health Quality [NICHQ] Vanderbilt Assessment Scales,” says Wolf. For that, you will report 96127 (Brief emotional/behavioral assessment (eg, depression inventory, attention-deficit/hyperactivity disorder [ADHD] scale), with scoring and documentation, per standardized instrument). Expert Tip 2: Knowing This Coding can Help Coding for ADD can be a source of great confusion. That’s because, if you go to the ICD-10 alphabetical index, the entry for “Disorder, attention-deficit without hyperactivity (adolescent) (adult) (child)” directs you to F98.8. However, this may not be the correct way to code the diagnosis. In fact, “the term ‘ADD’ is considered outdated,” according to Wolf. “The Diagnostic and Statistical Manual of Mental Disorders [DSM] lists three types of ADHD: predominantly inattentive presentation, which is coded as F90.0 in ICD-10; predominantly hyperactive-impulsive presentation, which is coded as F90.1 in ICD-10; and combined presentation, which ICD-10 codes to F90.2. The first type of ADHD is what providers used to refer to as ‘ADD,’” Wolf believes. “It is clear that the intent of DSM was to remove the term ADD and create new subtypes that streamline the coding of this disorder and specifically cross-walk to the ICD-10 F90 series,” agrees Donna Walaszek, CCS-P, billing manager, credentialing/coding specialist for Northampton Area Pediatrics LLP, in Northampton, Massachusetts. So, unless your pediatrician or payer expresses a clear preference for coding ADD to F98.8, you should steer clear of that code and use F90.0 instead. Expert Tip 3: Don’t Forget Common Coexisting Conditions Citing the 2007 National Survey of Children’s Health (NCSH), the organization Children and Adults with Attention-Deficit/Hyperactivity Disorder (CHADD) notes that “33 percent of the children with ADHD had one coexisting condition, 16 percent had two, and 18 percent had three or more” (Source: chadd.org/for-professionals/coexisiting-conditions/). So, there’s a pretty good chance you will be called on to document additional diagnoses. “When this happens, decisions regarding which disorder to treat first depend on the impairment of the symptoms in the patient’s life. It is always important to report all coexisting disorders when the status of the disorder is addressed,” says Walaszek.