Focus Your ED ICD-10 Prep on These Top-9 Codes, Part 1
Set yourself up for diagnosis success this fall.
Without the correct diagnosis codes to support your emergency department (ED) visit codes, you’ll face denials — and starting in October with the transition to ICD-10, your job will get a bit harder. But if you prepare now and learn the top diagnosis codes you’ll attach to your ED claims, you can be ready for the fall changes.
Check in: By now your coding team should be proficient in ICD-10 and demonstrate that proficiency by coding parallel to ICD-9 (or dual coding) on live charts that go through an internal audit process, advises Caral Edelberg, CPC, CPMA, CAC, CCS-P, CHC, Chairman, Edelberg & Associates. This gives each coder an opportunity to fine-tune any areas that require additional focus and remediation.
Streamline your ICD-10 prep with this helpful instruction from Edelberg on these top emergency medicine diagnosis areas. Review the first four this month and stay tuned to next month’s Evaluation & Management Coding Alert for the last five.
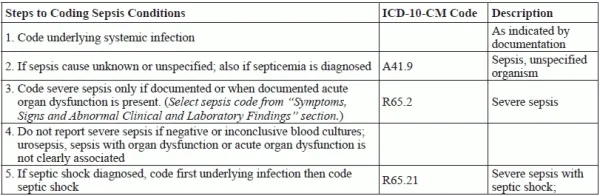
1. Dig into the Details for Sepsis
When an infection is the principle diagnosis, report it first, followed by the non-infectious condition such as burn, trauma, etc. The chart on the next page summarizes your choices.
2. Focus on Type for Dementia
Dementia is characterized by the development of multiple cognitive deficits such as memory impairment and cognitive disturbances, including aphasia, apraxia, and agnosia, which are coded to the Mental, Behavioral and Neurodevelopmental disorders (FXX) code set, says Edelberg. Alzheimer’s (G30) and Parkinson’s disease (G20) related dementia are coded first as the underlying disease, followed by the type of impairment, e.g. Dementia at F02.8.
Dementia, classified in subcategory F02.8, is due to direct physiological effects of a general medical condition, she confirms. If the patient has wandered off, Z91.83 would be assigned to the F02.81 or F03.91.
3. Specify Dominance with Hemiplegia and Hemiparesis
When identifying hemiplegia and hemiparesis, you should note whether the dominant or non-dominant side is affected, advises Edelberg. The official ICD-10-CM coding guidelines indicate that should the affect side be documented, but not specified as dominant or non-dominant, and the classification system does not indicate a default, your code selection should be considered as follows;
4. Skip General Pain Dx If You Have Specifics
If the definitive diagnosis is known, do not report pain unless the reason for the encounter is pain control or management of pain and not for the treatment of the underlying condition, says Edelberg. The site of the pain is coded from Chapter 18, Signs, Symptoms and Abnormal Clinical and Laboratory Findings, Not Elsewhere Classified. If the pain is documented as acute or chronic, category G89 is appropriate, she notes.
Codes from G89 are generally reported first, followed by the site if the encounter is specifically for pain management, says Edelberg. If the encounter is for a condition other than pain control or pain management without a definitive diagnosis, assign a code for the site of the pain first followed by a code from the G89 category.
Chronic pain is reported with G89.2x. It requires specific documentation that the pain is, indeed, chronic. There is no time frame for classifying pain as chronic, says Edelberg.
The terminology for epilepsy has been updated, with terms to classify the disorder such as:
Neoplasm related pain is coded with G89.3 and can be coded without acute or chronic status documented.