Double Check Your Time Statement before Assigning a Critical Care Code
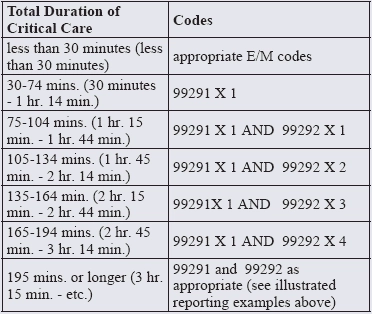
Verify your time attestation statement for the best results. Critical care coding is an ever increasing major audit target and these claims tend to receive the closest scrutiny from claims reviewers. And the bad news doesn't end there. Caution: Some payers are going to prepayment audits to make sure the documentation is correct before paying for 99291 (Critical care, evaluation and management of the critically ill or critically injured; first 30-74 minutes). The ED E/M codes reported in the ED are assigned and audited using documentation guidelines. But that's not the case for the critical care codes. As a result, these codes can be misunderstood by those unfamiliar with the rules that do apply. Check out these expert tips on what "critical" actually means and which services are, and are not, bundled into the critical care codes. How is Physician Time Measured for the Purpose of Reporting Critical Care? The duration of critical care services for both CPT® and Medicare is based on the physician's documentation of total time spent evaluating, managing, and providing care to the critical patient, as well as time spent in documenting such activities. The physician must devote full attention and be immediately available to the particular patient for every minute of time claimed. This time may be spent at the patient's immediate bedside or elsewhere on the unit, as long as the physician is immediately available to the critically ill or injured patient, says Michael A. Granovsky, MD, FACEP, CPC, President of Logix Health, a national ED coding and billing company based in Bedford, MA. For example: Time spent can be at the bedside, reviewing test results, discussing the case with staff, documenting the medical record, and time spent with family members (or surrogate decision makers) discussing specific treatment issues when the patient is unable or clinically incompetent to participate in providing history or making management decisions. Take note: When the provider performs separately reportable procedures or services, you cannot count that time as part of the total time you report as critical care time. You also can't count time involved in activities like restocking of supplies that do not directly contribute to the treatment of the critical patient toward the critical care time. The critical care codes 99291 and 99292 are used to report the total duration of time spent by a physician providing critical care services, even if the time spent by the physician on that date is not continuous. You can aggregate non-continuous time for critical care services for a single date. Use CPT® code 99291 to report the first 30-74 minutes of critical care on a given date. This code should be used only once per date. Use code 99292 to report additional block(s) of time of up to 30 minutes each beyond the first 74 minutes of critical care. Don't use the critical care codes to report critical care time of less than 30 minutes. Instead, report such service the appropriate E/M code, likely 99285 based on the nature of the presenting problem documented, states Granovsky The time based critical care codes (99291 and 99292) are appropriate to use when reporting services in the ED. The critical care neonatal (99468-99469) and pediatric (99471, 99472, 99475 and 99476) codes describe services by the day rather than by the hour or half hour and are used in the inpatient setting, he adds. What's the Midpoint Threshold, Is It 30 or 31 Minutes to Qualify For Critical Care? The CPT® book introduction discusses time threshold requirements for code sets that contain a time basis for code selection. "The following standards shall apply to time measurement, unless there are code or code-range-specific instructions in guidelines, parenthetical instructions, or code descriptors to the contrary. A unit of time is attained when the mid-point is passed. For example, an hour is attained when 31 minutes have elapsed (more than midway between zero and sixty minutes). A second hour is attained when a total of 91 minutes have elapsed," the manual advises. In the case of code 99291, there is specific language in CPT® that states 30 minutes both in the code descriptor itself and in the time threshold chart in the critical care section preamble. So for 99291, CPT® describes a threshold of at least 30 minutes, when the midpoint would have been passed, Granovsky explains. Consider this example: A patient presents to the ED with worsening chest pain. The physician examines the patient and finds him to have elevated blood pressure and tachycardia. The patient is started on a Cardizem drip to control his heart rate. Labs, chest x-ray, and an EKG are ordered. Multiple re-evaluations are performed. The physician interprets both the x-ray and EKG, and the patient is diagnosed with CHF and atrial fibrillation. The EKG interpretation takes the physician five minutes, and the rest of the encounter took 50 minutes. Make sure you have your time thresholds by using this chart from the CPT® coding manual In this example, the physician spent 50 minutes providing critical care services to this patient (this time excludes time spent interpreting the EKG). On the claim you would: On this claim, you would not code the chest x-ray interpretation, as it is bundled into the critical care code, says Granovsky. Of note: Be sure to deduct the time spent providing these separately billable procedures from your critical care time reported, states Granovsky. Payers May Challenge Whether Your Patient Was Really Critically Ill or Injured Aside from clear documentation of the aggregate critical care time, whether the patient was critically ill or injured is perhaps the most important question you'll need to answer on any critical care claim. You must be able to establish that the patient is critically ill or injured to report 99291. CPT® defines critically ill or injured as "an injury or illness that acutely impairs one or more vital organ systems such that there is high probability of imminent or life threatening deterioration in the patient's condition," says Granovsky. He offers these examples of patients that insurers would consider critically ill or injured: Can You Defend The "High Probability" Clause? Although most critical patients in the emergency department are actively critically ill or injured, some may just be potentially unstable to the point that they will very likely become unstable without immediate treatment. When determining whether or not a patient is critically ill or injured, the physician should consider the likelihood that they would have a clinically significant deterioration if nothing was done in the next hour. If the probability for imminent or life threatening deterioration is high, critical care may be an appropriate consideration. For example consider a patient with an allergic reaction with severe laryngeal swelling that threatens to close off his airway, but is not yet fully decompensated and requiring intubation, says Granovsky. Go By The Book: Teaching Physicians Must Meet Higher Critical Care Documentation Standards The teaching physician section in the Centers for Medicare and Medicaid Services critical care Transmittal 1548 from July 2008, has specific language relating to the requirements for teaching physicians reporting of critical care services, says Granovsky. This transmittal seems to hold the teaching physician documentation of critical care to a specific standard and set of time counting criteria. "For CPT® codes determined on the basis of time, such as critical care, the teaching physician must be present for the entire period of time for which the claim is submitted," CMS advised in the transmittal. Section M of Transmittal 1548 goes on to state "Time spent teaching may not be counted towards critical care time. Time spent by the resident, in the absence of the teaching physician, cannot be billed by the teaching physician as critical care or other time-based services. Only time spent by the resident and teaching physician together with the patient or the teaching physician alone with the patient can be counted toward critical care time." Example: CMS provides the following example of acceptable teaching physician documentation. "Patient developed hypotension and hypoxia; I spent 45 minutes while the patient was in this condition, providing fluids, pressor drugs, and oxygen. I reviewed the resident's documentation and I agree with the resident's assessment and plan of care." Vital: Remember that a resident's work and time providing critical care services cannot be used by the teaching physician to support reporting critical care. Teaching Time On Its Own Doesn't Count "Time involved in activities that do not directly contribute to the treatment of the critically ill or injured patient may not be counted towards the critical care time, even when they are performed in the critical care unit at a patient's bedside (e.g., review of literature, and teaching sessions with physician residents whether conducted on hospital rounds or in other venues)," CMS states in Transmittal 1548, Section E.5, under Inappropriate Use of Time for Payment of Critical Care Services. In other words, you cannot count time spent in teaching above and beyond the provision of critical care to the patient. However, the transmittal statement does not mean that any critical care event that might involve a resident does not count, Granovsky explains. Check With Payers Before Submitting Claims With Both ED E/M and Critical Care CPT® is clear in stating that critical care and other E/M services may be provided to the same patient on the same date by the same physician. However Medicare does not agree with that policy. CMS specifically addresses this question in Transmittal 1548, with regard to the emergency department. When a patient requires critical care services upon arrival into the emergency department, only critical care codes (99291-99292) may be reported, according to the transmittal. An emergency department E/M code (99281-99285) by the same provider/group on the same date is not reported in addition to those services, says Granovsky. The Order of the Codes Doesn't Matter It does not matter if the critical care precedes or follows what would normally be an E/M service in the emergency department. Transmittal 1548 clearly states that hospital emergency department services are not payable for the same calendar date as critical care services when provided by the same physician (which includes any physician of the same specialty in the same group) to the same patient. So, if a Medicare patient presents to the emergency department and receives a Level 5 ED E/M workup, and later in the shift unexpectedly clinically deteriorates requiring critical care services, according to CMS, the "same" ED physician would typically report only the critical care service - but not both, Granovsky explains.