
Wield Your Imaging Edge With the New X-ray CPT® Codes for 2016
Enjoy wider range of Code choices for spinal X-rays.
There’s a lot to learn from additions to the CPT® code set this year if you take X-rays of patients in your practice. X–rays, or radiographs, involve using radiation to diagnose, manage, and treat diseases by examining specific body structures, and form a major body of evidence for proving medical necessity for chiropractic treatments, alongside the P.A.R.T assessment.
“Providers do take x-rays in the practice as it helps to determine a plan of treatment quicker and more efficiently because they are being done in the same visit,” says Doreen Boivin, CPC, CCA, with Chiro Practice, Inc., in Saco, Maine. “Otherwise, the provider would have to send them to the hospital and wait for results. For a patient in pain this can make a significant difference.”
Get Your Feet Wet in the Spinal X-Ray Codes Reshuffle
CPT® 2016 adds 72801 for full spine single view, and three successive codes for additional views to replace 72090 (Radiologic examination, spine; scoliosis study, including supine and erect studies). At this time, CPT® does not provide an indication as to the reason for deletion of this code. Here are the new code descriptors in detail:
Report 72081 to report a single plain X-ray image of the entire thoracic and lumbar spine taken from a single angle or direction (projection). The single image may include the skull, neck (cervical spine), and tailbone (sacral spine). So, if included, do report a separate code. The procedure is typically performed to evaluate a patient for scoliosis, an abnormal curvature of the spine that is oriented from side to side.
If the provider takes two or three views of the back, use code 72082; for four or five views of the back, use code 72083; and if the provider takes at least six views of the back, use code 72084.
Know the All New Hip and Pelvis X-ray Codes, Too
It’s generally thought that because extraspinal procedures are not covered, DCs would not be dealing much with the limbs. Just how applicable are these codes to DCs?
“Everything is connected,” explains Boivin. “The provider will do all that is needed to make sure the patient is taken care of.”
CPT® 2016 adds 73521, 73522, 73523 (Radiologic examination, hips, bilateral, with pelvis when performed; with 2 views, 3-4 views, and minimum of 5 views respectively) to replace 73520 (Radiologic examination, hips, bilateral, minimum of 2 views of each hip, including anteroposterior view of pelvis), which was never assigned a Relative Value Scale. You can use the new codes based on the number of views taken to report plain X-rays of both or bilateral hips, and pelvis if included, from two or more different projections or directions. In this diagnostic procedure, the provider takes two or more X–ray images from different projections (directions or angles) of both hips, left and right, to check for fracture, swelling, or other reason for pain in the hip area. The procedure may include the entire pelvis, which includes the hip bone, the sacrum (the large triangular bone at the lower end of the spinal column) and the coccyx or tailbone.
New Unilateral Hip X-ray Codes: Amongst the new codes added, we also have 73501(Radiologic examination, hips, unilateral, with pelvis when performed; one view), which is a unilateral hip x-ray that includes the pelvis. Now, this is a one view, and it is used to report a single X-ray of one hip, and thus is unilateral. Code 73502 is for a unilateral hip and pelvis with two or three views such as AP and lateral. 73503 is a unilateral hip with the pelvis, including four plus views. Here are the code descriptors in detail:
For plain X–rays of the pelvis, see 72170 (Radiologic examination, pelvis; 1 or 2 views) and 72190 (Radiologic examination, pelvis; complete, minimum of 3 views). Codes 72170 and 72190 continue to be available for use.
Femur specific codes: In case you just wanted to focus on the femur, we have a couple of new codes for that. CPT® 2016 adds 73551(Radiologic examination, femur; 1 view) to report a single X-ray of the femur exclusively, for which there was no previous code. You can use 73551 to report a single plain X-ray of the left or right femur, but not both. Again, this code does not include the pelvis.
In this diagnostic procedure, the provider takes an X–ray image from a single projection (direction or angle) of the femur, or thigh bone, to check for fracture, swelling, or other reason for pain in the thigh area. If the provider examines at least two views of the thigh bone, use code 73552 (Radiologic examination, femur; minimum 2 views).
Step Out Of the Shadows of Deleted Codes
Let’s move on to codes that you can no longer report because they’ve been deleted. Get them out of your billing system and erase them from your superbill.
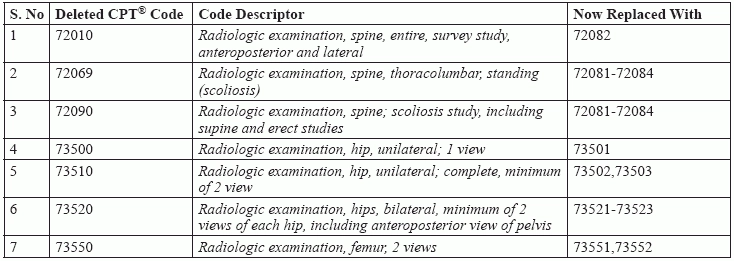
Here is a quick list of the obsolete codes, along with their code descriptors and the codes to use for each scenario now.
Taking a look at the deleted code 72010, a full spine survey with two views, we know that the code for this is the brand new 72082. Next, we move on to 72069, a thoracolumbar standing scoliosis study, and 72090, the scoliosis study, these again are going to be replaced by the additions 72081-84. Further on, needless to say, the table depicts the changes you need to save to memory.
Pay Attention to Documentation Details
So, how do you make the most of this new development? Here are a few tips on getting the most out of these changes:
1) If you are reporting only the physician’s interpretation for the radiology service, append modifier 26 (Professional component) to the radiology code.
“Follow the steps and you won’t go wrong,” assures Boivin. “You will get reimbursed the reasonable and customary amount by the payers.”
Final takeaway: As of now, although there are more changes to the CPT® code set, they do not relate to a typical chiropractic setting.
“Make sure to have the resources available at arm’s length or just by picking up the phone,” advises Boivin. “Don’t hesitate to ask for help.”
Focus on getting these codes right, so that you can reap the benefits of a smooth reimbursement.
2) If you are reporting only the technical component for the radiology service, you should append modifier TC (Technical component) to the radiology code unless the hospital provided the technical component. In that case, do not append modifier TC because the hospital’s portion is inherently technical.
3) Moreover, do not append a professional or technical modifier to the radiology code when reporting a global service in which one provider renders both the professional and technical components.
4) Be sure that the provider’s documentation clearly describes each view taken in a radiology service.
5) Check the documentation for the patient’s body position and projection of the X–ray to assign the correct number of views.



