What is medical coding?
Medical coding is the transformation of healthcare diagnosis, procedures, medical services, and equipment into universal medical alphanumeric codes. The diagnoses and procedure codes are taken from medical record documentation, such as transcription of physician's notes, laboratory and radiologic results, etc.
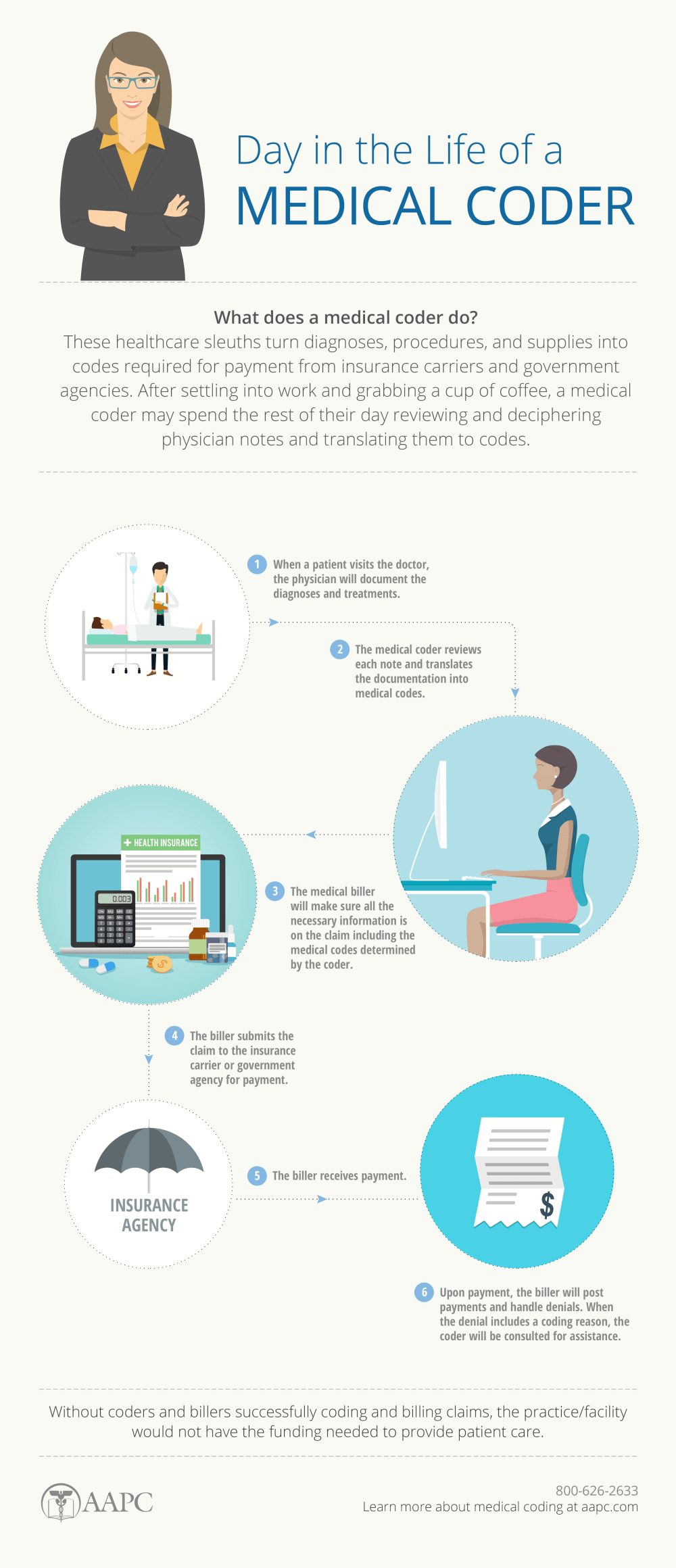
Medical coding professionals help ensure the codes are applied correctly during the medical billing process, which includes abstracting the information from documentation, assigning the appropriate codes, and creating a claim to be paid by insurance carriers.
Medical coding happens every time you see a healthcare provider. The healthcare provider reviews your complaint and medical history, makes an expert assessment of what’s wrong and how to treat you, and documents your visit. That documentation is not only the patient’s ongoing record, it’s how the healthcare provider gets paid.
Medical coders translate documentation into standardized codes that tell payers the following:
Patient's diagnosis
Medical necessity for treatments, services, or supplies the patient received
Treatments, services, and supplies provided to the patient
Any unusual circumstances or medical condition that affected those treatments and services
Like a musician who interprets the written music and uses their instrument to produce what's intended, medical coding requires the ability to understand anatomy, physiology, and details of the services, and the rules and regulations of the payers to succeed. Check out our webinar to learn more — Guidelines: The Foundation of Coding.
Medical coding derives from public bills of mortality posted in London in the 18th century. It was through correlating these that doctors determined the cause of a cholera epidemic. It is even more vital now as the data gathered through medical coding is used to improve healthcare overall. The results are submitted to payers for reimbursement, but the data derived from the codes also are used to determine utilization, manage risk, identify resource use, build actuarial tables, and support public health and actions.

Medical coding requires a particular discipline. Medical coders are considered part of the medical team, often working very closely with providers, management, and payers. A scholar, detective, educator, and problem solver, medical coders possess particular skills.
The medical coder and biller process a variety of services and claims on a daily basis. Medical codes must tell the whole story of the patient's encounter with the physician and must be as specific as possible in capturing reimbursement for rendered services. To better understand what a coding transaction looks like, read the article: What does a medical coder do?
The main task of a medical coder is to review clinical statements and assign standard codes using CPT®, ICD-10-CM, and HCPCS Level II classification systems. Medical billers, on the other hand, process and follow up on claims sent to health insurance companies for reimbursement of services rendered by a healthcare provider.
The medical coder and medical biller may be the same person or may work with each other to ensure invoices are paid properly. To help promote a smooth coding and billing process, the coder checks the patient’s medical record (i.e., the transcription of the doctor’s notes, ordered laboratory tests, requested imaging studies, and other sources) to verify the work that was done. Both work together to avoid insurance payment denials.
Why is medical coding needed?

The healthcare revenue stream is based on the documentation of what was learned, decided, and performed.
A patient's diagnosis, test results, and treatment must be documented, not only for reimbursement but to guarantee high quality care in future visits. A patient's personal health information follows them through subsequent complaints and treatments, and they must be easily understood. This is especially important considering the hundreds of millions of visits, procedures, and hospitalizations annually in the United States.
The challenge, however, is that there are thousands of conditions, diseases, injuries, and causes of death. There are also thousands of services performed by providers and an equal number of injectable drugs and supplies to be tracked. Medical coding classifies these for easier reporting and tracking. And in healthcare, there are multiple descriptions, acronyms, names, and eponyms for each disease, procedure, and tool. Medical coding standardizes the language and presentation of all these elements so they can be more easily understood, tracked, and modified.
This common language, mandated by the Health Information Portability and Accountability Act (HIPAA), allows hospitals, providers, and payers to communicate easily and consistently. Nearly all private health information is kept digitally and rests on the codes being assigned.
Types of codes used
Medical coding is performed all over the world, with most countries using the International Classification of Diseases (ICD). ICD is maintained by the World Health Organization and modified by each member country to serve its needs. In the United States, there are six official HIPAA-mandated code sets serving different needs.
ICD-10-CM (International Classification of Diseases, 10th Edition, Clinically Modified)
ICD-10-CM includes codes for anything that can make you sick, hurt you, or kill you. The 69,000-code set is made up of codes for conditions and disease, poisons, neoplasms, injuries, causes of injuries, and activities being performed when the injuries were incurred. Codes are “smart codes” of up to seven alphanumeric characters that specifically describe the patient’s complaint.
ICD-10-CM is used to establish medical necessity for services and for tracking. It also makes up the foundation of the MS-DRG system below.
CPT® (Current Procedure Terminology)
This code set, owned and maintained by the American Medical Association, includes more than 8,000 five-character alphanumeric codes describing services provided to patients by physicians, paraprofessionals, therapists, and others. Most outpatient services are reported using the CPT® system. Physicians also use it to report services they perform in inpatient facilities. Here's a little behind the scene on the making of CPT® codes.
ICD-10-PCS (International Classification of Diseases, 10th Edition, Procedural Coding System)
ICD-10-PCS is a 130,000 alphanumeric code set used by hospitals to describe surgical procedures performed in operating, emergency department, and other settings. Don’t let the procedural coding intimidate you by taking the right approach to ICD-10-PCS coding.
HCPCS Level II (Health Care Procedural Coding System, Level II)
Developed originally for use by Medicare, Medicaid, Blue Cross/Blue Shield, and other providers to report procedures and bill for supplies, HCPCS Level II’s 7,000-plus alphanumeric codes are used for many more purposes, such as quality measure tracking, outpatient surgery billing, and academic studies.
CDT® (Code on Dental Procedures and Nomenclature)
CDT® codes are owned and maintained by the American Dental Association (ADA). The five-character codes start with the letter D and used to be the dental section of HCPCS Level II. Most dental and oral procedures are billed using CDT® codes.
NDC (National Drug Codes)
The Federal Drug Administration's (FDA) code set is used to track and report all packages of drugs. The 10-13 alphanumeric character smart codes allow providers, suppliers, and federal agencies to identify drugs prescribed, sold, and used.
Modifiers
CPT® and HCPCS Level II codes use hundreds of alphanumeric two-character modifier codes to add clarity. They may indicate the status of the patient, the part of the body on which a service is being performed, a payment instruction, an occurrence that changed the service the code describes, or a quality element.
MS-DRG and APC
Two federal code sets used to facilitate payment deriving from those above systems are MS-DRG and APCs. They rely on existing codes sets but indicate the resources consumed by the facility to perform the service.
MS-DRG (Medical Severity Diagnosis Related Groups)
MS-DRGs are reported by a hospital to be reimbursed for a patient’s stay. The MS-DRG is based on the ICD-10-CM and ICD-10-PCS codes reported. They are defined by a particular set of patient attributes which include principal diagnosis, specific secondary diagnoses, procedures, sex, and discharge status. The Centers for Medicare & Medicaid Services (CMS) work with 3M HIS to maintain this data set.
APC (Ambulatory Payment Categories)
APCs are maintained by the Centers for Medicare & Medicaid Services (CMS) to support the Hospital Outpatient Prospective Payment System (OPPS). Some outpatient services in a hospital, such as minor surgery and other treatments, are reimbursed through this system.
How is medical coding done?
Medical coding is best performed by trained and certified medical coders. The following example outlines what a typical day in the life of a Medical Coder may look like.
After settling into the office and grabbing a cup of coffee, a medical coder usually begins the workday by reviewing the previous day's batch of patient notes for evaluation and coding. The type of records and notes depends on the clinical setting (outpatient or facility) and may require a certain degree of specialization (Healthcare systems may have individuals who focus on medical specialties while coders who work in smaller, or more general offices, may have a broad range of patients and medical conditions.).
Selecting the top patient note or billing sheet on the stack, the coder begins reviewing the documentation to understand the patient's diagnoses assigned and procedures performed during their visit. Coders also abstract other key information from the documentation, including physician names, dates of procedures, and other information.
Coders rely on ICD-10 and CPT® code books to begin translating the physician's notes into useful medical codes. An example of basic procedure documentation and subsequently assigned codes can be seen below.
Many cases are simple to code. Individual medical coders develop a detailed understanding of the procedures and commonality of their specific clinic or facility. Coders occasionally encounter a difficult note requiring in-depth research, taking more time to code correctly. Even among the more commonly used codes are significant gray areas open for examination among coders. With very complex or unusual cases, coding guidelines may be confusing to interpret. Experienced coders will rely on their network of peers and professionals to discuss nuances in online forums, networking with specialists they have met at national conferences, or consulting with co-workers to help understand the issue and determine the proper codes. Ongoing training and current coding-related periodicals such as AAPC the Magazine also provide important opportunities to advance understanding and professionalism.
Finally, the coder completes the chart and begins the next patient record. This cycle of reading, note taking, assigning codes, and computer entry repeats with each chart. Most coders will spend the majority of their day sitting at the computer reading notes and using their computer to enter data into a billing system or search for information to clarify the documentation in the notes.
Here's an example of a case:
This is a 40-year-old male with rectal pain, rectal bleeding, and some left-sided lower abdominal pain. The colonoscopy procedure and the risks, not limited to bleeding, perforation, infection, side effects from medication, need for surgery, etc., and were fully explained to the patient. An informed consent was taken.Instrument Used: CF-Q160.
Sedation: Versed 5 mg IV in incremental doses and Demerol 100 mg IV in incremental doses performed by the anesthesia team.
Extent of Exam: Up to cecum as identified by ileocecal valve and appendiceal orifice.
Length of Scope Insertion: 110 cm.Postop Diagnoses/Impression:
1. Moderate-sized, internal hemorrhoids.
2. Mild diverticulosis.Description of Procedure: With the patient being in the left lateral position, first digital examination of the rectum was done, which was unremarkable. Then, the CF-Q160 was passed through the rectum under direct visualization and advanced all the way to cecum. The cecum was identified by ileocecal valve and appendiceal orifice. There were a couple of tics/diverticula seen on the left side of the colon. A careful look was taken while withdrawing the scope. Retroflex view in the rectum showed moderate-sized internal hemorrhoids.
Plan:
1. Anusol-HC suppositories for hemorrhoids.
2. High-fiber diet.
3. If there is no family history, a follow-up colonoscopy in 10 years.CPT® Code: 45378
ICD-10-CM Codes: K64.8, K57.30
How do you become a medical coder?
Successful medical coders know anatomy, physiology, medical procedures, and payer rules and policies. To become a medical coder, you must attend training via a coding-specific training program or college. Afterward, finding a job in the field is easier if you have a professional credential, such as AAPC's.
There are several medical coding certifications available, depending on the area of the revenue cycle you wish to pursue. The baseline for most is the Certified Professional Coder (CPC) , which certifies the coder’s ability to work in outpatient settings. Facility coders should pursue the Certified Inpatient Coder (CIC) for inpatient coding and Certified Outpatient Coder (COC) for hospital patients receiving in-and-out services. Here’s an infographic to help you chose the right hospital credential. There are several programs available both for online training on medical coding and physical medical coding training classes.
Today more than 200,000 medical professionals are members of AAPC. AAPC elevates the standards of medical coding by developing training, professional certification, opportunities to network with other related medical professionals and providing a variety of job search and career building opportunities.
Professional coders largely work independently. However, interaction with coding staff, medical billers, physicians, and ancillary office staff is essential. Medical coders are usually placed on tight production schedules and expected to complete a determined number of notes each day or to keep their lag days at a specified timeframe. Lag days are the number of days it takes for the notes to be documented to the actual claims submission date. The prime date is usually between two to five days.
Depending on the clinical setting, internal or external auditors periodically perform audits of the coding and documentation for accuracy and completeness. The results of these coding audits are maintained by the compliance department or the department supervisor and are a significant part of job evaluations.
How much does a medical coder make in a year?
AAPC-certified medical coders make $60,917 per year on average — 29% more than uncertified health information technicians who earn approximately $47,200 annually. Where you live, what role you play in the revenue cycle, and how much education and credentials you have can influence your pay. Coders who pursue career advancement, earning their Certified Professional Medical Auditor (CPMA), Certified Physician Practice Manager (CPPM), or Certified Documentation Expert Outpatient (CDEO) make average salaries of $71,646 annually, according to AAPC's 2024 Medical Coding Salary Survey.
Charting your career requires curiosity, continuing education, and imagination. Achieving the credential is the beginning of a lifetime of new experiences and knowledge.
About the author

Get certified as a professional coder with the CPC credential.
The CPC credential is the gold-standard credential for medical coders. AAPC's CPC Certification Preparation Course is an entry-level course that prepares you to take your CPC exam.
Certified Professional Coder (CPC)®
The CPC credential is the gold-standard credential for medical coders. It demonstrates expertise in coding medical services and procedures performed by physicians.